Colon adenocarcinoma is a malignant tumor that develops from the glandular epithelium. In the structure of all oncological neoplasms of the large intestine, it ranks first, accounting for up to 95% of cancers of this localization.
- Causes of development of colon adenocarcinoma
- Classification of colon adenocarcinoma
- Symptoms of adenocaricnoma of the colon
- Examination for adenocarcinomas of the large intestine
- Diagnosis of colon adenocarcinomas
- Treatment of colon adenocarcinoma
- Metastasis of adenocarcinoma
- Complications of colon adenocarcinoma
- Forecast
Causes of development of colon adenocarcinoma
The reasons for the development of adenocarcinoma are not completely clear, but there is some data that allows us to identify risk factors that increase the likelihood of developing this pathology:
- The nature of the diet is excessive consumption of animal fats, high-protein foods and lack of fiber in the diet, as well as overeating and alcohol abuse.
- Presence of colon polyps. In most cases, adenocarcinomas develop from existing polyps, and the longer it exists and the larger its size, the higher the risk of malignancy. In many countries, people over a certain age (50 years) are recommended to undergo periodic colonoscopy with simultaneous removal of polyps. Today this is the most effective means of prevention.
- Genetic predisposition. In most cases, colon adenocarcinoma is a sporadic disease, i.e., not associated with hereditary factors, but there are two cases where genetics play a key role. These are familial adenomatous polyposis and hereditary non-polyposis colon cancer (also known as Lynch syndrome).
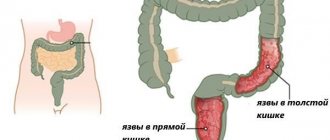
- The presence of nonspecific ulcerative colitis and Crohn's disease.
- A history of cancer of the female genital organs.
- Immunodeficiency states.
Causes
Colon damage is a type of colorectal cancer. Today, doctors cannot say what the exact cause of the development of pathology is. There are certain factors that provoke the malignant process of neoplasm development:
- Disturbances in the intestines associated with the disease. This may be polyposis, benign tumors.
- Eating disorder. Predominance of fatty foods, spicy and salty foods in the diet, reduction in the amount of fiber products.
- Consumption of alcohol and smoking in doses exceeding the body's regenerative powers.
- The workplace involves regular contact with toxic chemicals.
- Inheritance by clan. If your family or close relatives have suffered from cancer, the risk of developing the disease is high.
- Lack of bowel movements for a long time, presence of fecal stones that can form inside.
- The lifestyle involves constantly being in a sitting position, which provokes stagnation in the intestines.
The transformation of a benign tumor into cancer occurs quickly due to insufficient supply of blood and oxygen to the damaged cells. Other factors can also have an influence.
Classification of colon adenocarcinoma
Depending on the histological type, the following types of adenocarcinomas are distinguished:
- Tubular. Consists of specific tubular structures. The tumor, as a rule, is small in size and has unclear boundaries.
- Mucinous. Characterized by the secretion of large amounts of mucus. Histological examination shows that mucus occupies up to half the volume of malignant cells. The tumor belongs to poorly differentiated forms of adenocarcinoma, characterized by rapid growth and early metastasis.
- Signet ring cell. Also refers to a high degree of malignancy; at the time of diagnosis, distant metastases are usually detected. More often diagnosed in young people.
Depending on the degree of maturity of tumor cells, adenocarcinomas are divided into the following types:
- Well-differentiated adenocarcinoma. It is characterized by a relatively “normal” structure of cells in which an increase in the size of the nuclei is noted. Cellular functions are preserved. The tumor has a relatively favorable prognosis because it grows slowly. But at the same time, it is difficult to diagnose in the early stages, since the cells are externally similar to normal tissue.
- Moderately differentiated adenocarcinoma is characterized by a more unfavorable prognosis. The cells are polymorphic, prone to rapid division and, as a result, rapid tumor growth.
- Poorly differentiated and undifferentiated adenocarcinoma are most unfavorable. The cells are characterized by high polymorphism, the tumor does not have clear boundaries, infiltrates (grows) the intestinal wall and is characterized by rapid aggressive growth and early metastasis.
Depending on the prevalence of the tumor process, the following stages of adenocarcinoma are distinguished:
- Stage 1 - cancer cells are found only in the mucous membrane of the intestinal wall.
- Stage 2 - the tumor grows through all layers of the intestinal wall.
- Stage 3 - cancer metastasizes to regional lymph nodes.
- Stage 4 - distant metastases are detected that affect internal organs.
Histological types of colon adenomas
There are 3 histological types of colon adenomas:
- Tubular;
- Tubular villous;
- Villous.
The separation criterion is the ratio of villous and tubular structures. Tubular adenoma of the colon - what is it? Microscopically, tubular adenoma is represented by proliferating adenomatous epithelium. The tumor consists of branching and significantly convoluted glandular tubes, longer than in the normal intestinal mucosa. In tubular adenoma, no more than 25% villous tissue is present. Tubular adenoma of the colon has a mucous membrane-covered base. It is represented by connective tissue, smooth muscle cells and blood vessels. Tubular adenomas have a stalk and a smooth lobulated surface. Less often they are located on a wide base. Creeping tubular adenomas, which protrude slightly above the surface of the mucous membrane, are very rare.
In tubular-villous adenomas, the number of villi increases, which can be detected both on the surface of the polyp and inside large glands. The glands lengthen, acquire an irregular shape, and fit tightly to each other. The degree of epithelial dysplasia increases. In tubular-villous adenoma, the percentage of villous tissue varies from 25 to 75%. The tumor consists of pronounced lobules and has small areas with villi or very small lobules.
Villous adenoma consists of thin finger-like outgrowths of the connective tissue of the lamina propria, which are covered with epithelium. In villous adenomas, a small number of glands and 75% of the villous component can be found. Macroscopically, villous adenomas have a wide base and a “shaggy” surface. There is a special histological type of colon adenoma - serrated adenoma. The tumor is close in structure to a hyperplastic polyp, but has the potential for malignancy.
Adenomatous epithelium belongs to the category of neoplastic. For this reason, each adenoma has signs of dysplasia of varying severity. Histologists distinguish 3 degrees of dysplasia of tubular adenoma of the colon:
- 1st degree – weak;
- 2 degrees – moderate;
- Grade 3 – severe.
Tubular adenoma of the colon with low grade dysplasia is a poorly differentiated tumor. It can transform into adenocarcinoma.
Symptoms of adenocaricnoma of the colon
Colon adenocarcinoma does not manifest itself for a long time. The first symptoms may appear when the tumor reaches a large size and affects other organs. In some cases, there are indirect signs of the presence of malignant neoplasms:
- Unexplained weight loss.
- Loss of appetite.
- Prostration.
- Anemia, which develops against the background of hidden bleeding from the tumor.
Symptoms are also determined by the location of adenocarcinoma. If the tumor is located in the right part of the colon, then, as a rule, the first symptoms observed are dyspepsia associated with disruption of the functioning of neighboring organs (stomach, pancreas, liver and gall bladder). Hidden bleeding is possible, against the background of which anemia and weakness develop. Since in this place the intestine has a wide lumen and liquid contents, obturation (blockage of the lumen) develops only in the last stages and then not in all cases. If the tumor is large, it can be felt through the abdominal wall.
The left part of the colon has a smaller diameter, and the intestinal contents have a denser consistency, so tumors of this location are more often manifested by intestinal obstruction. Stagnation of intestinal contents leads to increased processes of putrefaction and fermentation, which causes bloating and colicky pain. Constipation is replaced by diarrhea with foul-smelling stools. In some cases, blood may be found in the stool.
Symptoms
In the early stages of progression, this type of tumor does not cause symptoms, or they are too mild. In the majority of cases, the appearance of a neoplasm is a consequence of a previously occurring chronic disease of the large intestine, for example, inflammation of the rectosigmoid region. In this case, the symptoms may be regarded by the patient as an exacerbation of an existing illness. Possible symptoms of this pathology include:
- abdominal pain;
- nausea with vomiting;
- general weakness and fatigue;
- loss of appetite and decrease in overall body weight;
- the occurrence of diarrhea;
- bloating;
- increased body temperature;
- impurities of blood and mucus in the stool.
All these signs are nonspecific and as the tumor develops, as well as the occurrence of metastases in the rectum and distant organs, their manifestations become more intense. Patients experience heaviness in the abdomen and frequent heartburn, and purulent discharge appears in the feces, which indicates significant intoxication.
We recommend reading: What is sarcoma and how does it manifest?
Examination for adenocarcinomas of the large intestine
The gold standard for detecting early-stage colon adenocarcinoma is a total colonoscopy. Experts from the European Oncology Clinic recommend doing it to all people over 50 years old once a decade. This will prevent existing benign polyps from becoming malignant. This method causes some discomfort to patients, so it is often performed under intravenous anesthesia. The cost of such an examination is quite high, and it also requires special preparation.
Patients are not always ready for this procedure, so there is a simpler and more affordable option, although less accurate - testing stool for occult blood. If the test result is positive, the patient is referred for a total colonoscopy.
Sample menu and diet for glandular colon cancer
Proper nutrition and diet for colon adenocarcinoma is one of the most important conditions for recovery. Patients should exclude a huge number of foods from their diet.
Useful foods for cancer of the digestive system: vegetables and fruits (pay attention to yellow, green and red root vegetables), herbs, carrot and beet juices, pureed soups, cereal porridges, pumpkin, boiled dietary meat, steamed omelet, cottage cheese, bread (bran), vegetable oil, green tea.
Prohibited foods for cancer of the digestive system: sugar, strong tea, coffee, alcohol, fried and fatty foods, smoked foods, sauces, seasonings, mushrooms, canned food, animal fat.
Healthy diet
Recommendations for taking food in the postoperative period:
- eating small portions;
- avoiding long breaks between meals;
- eat only pureed foods;
- do not drink or eat cold things, only warm ones;
- Food cannot be fried, only boiled or steamed;
- completely eliminate fermentation products.
The diet should include porridge with water, exclude spicy and salty foods. Preference should be given to lean soups, eating only fresh vegetables and fruits. The daily menu should be rich in fiber.
Sample menu in the postoperative period:
- 1 breakfast: still mineral water with lemon juice;
- 2nd breakfast: vegetables, fruits, nuts, kefir – ½ cup;
- Lunch: chicken broth soup, fresh vegetable salad, boiled lean fish or lean veal or chicken;
- Afternoon snack: fruit juice, whole grain bread;
- Dinner: baked vegetables;
- 2nd dinner: vegetable or fruit juice.
Diagnosis of colon adenocarcinomas
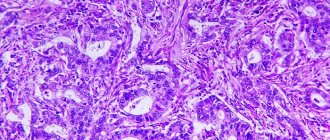
The diagnosis of colon adenocarcinoma is made only on the basis of a histological conclusion - an examination of a piece of tumor tissue under a microscope. The process of removing a piece of tissue is called a biopsy; it is performed using endoscopic technology during a colonoscopy. If the diagnosis is confirmed, further examination is prescribed, which is aimed at determining the histological type of the tumor and its molecular genetic features. A comprehensive examination is also carried out aimed at establishing the extent of the malignancy. For this purpose, CT, MRI, and ultrasound are performed. All together this will allow you to choose the optimal treatment tactics. Tests for tumor markers are also prescribed: CEA, CA19-9, CA-72-4. Although they do not help in detecting the tumor as such, tracking the dynamics of their concentration makes it possible to assess the effectiveness of further treatment and timely determine the recurrence of the disease.
Book a consultation 24 hours a day
+7+7+78
Symptoms and diagnostic signs
In addition to the general symptoms given above, you can add signs of an advanced stage of the disease:
- the tumor is palpable through the abdomen;
- there is a suspicion of peritonitis;
- when obstruction develops, the patient experiences vomiting of feces, cessation of gas discharge, and intense pain;
- accompanied by weakness, weight loss;
- Intestinal bleeding is often observed.
The most significant and informative diagnostic methods are:
- tumor markers;
- biopsy;
- histological studies;
- different options for endoscopy.
Identification of tumor markers are substances that naturally increase in concentration with a certain type of cancer; they are determined in venous blood. For intestinal cancer, it is determined:
- presence of tumor cells marker CA 19-9 and CEA for suspected rectal cancer;
- carcinoembryonic antigen.
Carrying out endoscopic examinations with the introduction of a sigmoidoscope, a fibrocolonoscope into the rectum, a laparoscope into the abdominal cavity, as well as the ability to examine tissue urgently during surgery gives clinicians a way to establish moderately differentiated growth of glandular cells. Suitable for cytology:
- fragments of fabric;
- imprints of the removed mucous membrane;
- purulent and mucous discharge.
The conclusion indicates the type of tumor as well- or low-differentiated adenocarcinoma of the colon or small intestine.
During a colorectal examination, the cancerous tumor is examined and a piece of tissue is removed for cytology.
Adenocarcinoma of the large intestine also differs in its histological structure; they are distinguished:
- dark cell tumor;
- mucinous;
- cancer without classification.
Treatment of colon adenocarcinoma
Surgery and chemotherapy are used to treat adenocarcinoma. If the tumor is located in the rectum, radiation therapy is possible.
Surgery
Surgical treatment involves removal of adenocarcinoma within healthy intestinal tissue. Depending on the volume of intestine removed, the following types of surgery are distinguished:
- Colon resection. The tumor is excised within healthy tissue. The ends are sutured to form an anastomosis.
- Hemicolectomy. Half of the large intestine is removed. Accordingly, right-sided and left-sided hemicolectomy are distinguished.
- Colectomy - the entire colon is removed.
If the tumor has spread to neighboring organs, a combined operation is performed to remove all affected tissues en bloc, following the rules of ablastics. As a rule, these are extensive traumatic interventions.
Distant single metastases (in the liver, lungs, ovaries) are also removed surgically, simultaneously with the main tumor or a separate operation, which is performed several weeks later. This issue is resolved by the council.
In some cases, after removal of adenocarcinoma, it is not possible to perform an anastomosis, then the overlying section of the intestine is removed to the abdominal wall, this is called a colostomy. It can be temporary or permanent. In the first case, some time after removal of the tumor, reconstructive interventions are performed to restore the integrity of the intestine.
An alternative to a colostomy can be endoscopic stenting - installation of a special structure that supports the intestinal lumen at the site of tumor damage in a straightened state. It can be performed in two versions:
- Preoperative decompression. It allows you to prepare the patient for a one-stage operation without a colostomy. Intestinal straightening eliminates intestinal obstruction, normalizes water and electrolyte balance and prepares the intestinal wall for anastomosis. In addition, stenting allows time for adjuvant chemotherapy, which will allow the tumor to shrink in size and allow surgery to be performed without removing a large amount of bowel.
- Palliative treatment - endoscopic stenting can be an alternative to a permanent colostomy or bypass for patients who, for some reason, cannot undergo surgery.
Chemotherapy
Chemotherapy for colon adenocarcinomas is carried out in two modes:
- Neoadjuvant, which is prescribed at the preoperative stage. Its purpose is to reduce the size of the tumor, making it easier to remove during surgery. Neoadjuvant therapy in some cases makes it possible to transfer a tumor from an unresectable state to a resectable state and to perform an operation that was initially impossible.
- The adjuvant regimen involves the use of chemotherapy in the postoperative period. Its goal is to destroy remaining cancer cells and prevent relapses of the disease.
There are several protocols for the chemotherapy treatment of adenocarcinoma, all of which include fluoropyrimidine-based cytostatics.
Targeted therapy can also be used, which acts on the molecular mechanisms that ensure tumor growth. Drugs that suppress the action of vascular endothelial growth factor (bevacizumab, ramucirumab) or epidermal growth factor receptor blockers (cetuximab) are used. Their appointment is carried out in accordance with molecular genetic testing.
Radiation therapy
Radiation therapy is used only in the treatment of adenocarcinomas of the rectum, since the remaining parts of the large intestine have high mobility, which does not allow marking the radiation field. Radiation therapy can be used preoperatively and postoperatively. In the first case, the goal is to reduce the tumor mass, and in the second, the destruction of cancer cells in the surrounding tissues.
Immunotherapy of adenocarcinoma in the presence of microsatellite instability
About 15% of cases of colon adenomas develop as a result of a breakdown of the mismatched nucleotide repair system - a special system that is designed to promptly recognize and eliminate DNA mutations. If it does not work, the genetic code is not protected and cells actively accumulate mutations, which are detected in repeating nucleotide sequences - microsatellites. This condition is called microsatellite instability. Tumors with this feature respond well to immunotherapy.
Normally, the immune system should destroy foreign cells and agents, but a cancer tumor manages to avoid this process with the help of special processes of interaction with the immune system. Immunotherapy blocks these processes and makes the tumor a visible target, allowing it to be destroyed. The Nobel Prize was awarded in 2021 for the development of this treatment method.
One of the immunological drugs is pembrolizumab. Its use can significantly improve the results of treatment of patients with metastatic colon adenocarcinoma, characterized by microsatellite instability.
Treatment
Therapeutic measures to combat adenocarcinoma depend on the results of the examination. Treatment of the disease is carried out using various methods. Positive results are shown by complex therapy, including surgery, chemotherapy, and radiotherapy. Diagnostics determines which technique to use and the duration of treatment.
Surgical intervention
When a cancerous tumor is detected, surgery is considered the main method of control. Surgery results in the removal of part of an organ or complete removal. When a patient is diagnosed with adenocarcinoma of the cecum, resection of the affected area with adjacent lymph nodes occurs. If the patient has rectal cancer, the colon and anal outlet must be removed.
After the operation, the patient begins a recovery period. During this time, physiotherapeutic procedures and medications are prescribed. An integrated approach promotes speedy recovery in the postoperative period. If there are contraindications to the operation, other methods are used.
Chemotherapy
For adenocarcinoma, surgery can be avoided. As a rule, chemotherapy is prescribed when metastases spread in the body. Also, this method can significantly prolong the life of a patient in the last stages of the disease.
Carrying out a chemotherapy procedure
Chemotherapy involves the introduction of special drugs into the tumor aimed at reducing the viability of cancer cells.
Radiation therapy
For patients at cancer centers, radiation therapy helps reduce the pain that occurs after surgery.
Radiation therapy is often the main method of combating adenocarcinoma. This occurs when the patient is contraindicated for resection of the affected organ.
More often, radiation therapy is part of complex treatment, allowing to reduce the spread of metastases in the body. It also helps reduce the risk of developing a recurrent reaction.
Metastasis of adenocarcinoma
Metastasis of adenocarcinoma is carried out in several ways:
- Lymphogenic - with the flow of lymph, tumor cells first enter the regional lymph nodes, and from there to more distant groups, for example, the supraclavicular.
- The hematogenous method of metastasis involves the dispersal of cancer cells through the bloodstream. Most often, metastases form in the liver (along the portal vein) and lungs. In poorly differentiated and undifferentiated adenocarcinomas, bone marrow damage is possible.
- If colon adenocarcinoma has invaded surrounding organs, implantation metastasis is possible as a result of contact of the tumor with the receiving surface. In this case, multiple metastases throughout the peritoneum (carcinomatosis) are possible.
What is intestinal adenocarcinoma?
Adenocarcinoma is an injury to the tissues of the intestinal tract by a malignant neoplasm that is formed from glandular epithelial cells.
This type of oncology is very dangerous due to its asymptomatic course up to almost 4 degrees of severity. The developing symptoms of the tumor are subtle and too typical for a large number of different diseases in the stomach and intestines. This greatly complicates the timely diagnosis.
Metastases of adenocarcinoma penetrate into nearby lymph nodes, the liver and lungs. Pathogenic cells are carried by the blood to healthy organs and tissues - this is how new foci are formed and multiple tumors are formed. An oncologist must carry out diagnosis and treatment.
In ICD-10, malignant neoplasms of the digestive organs are designated by codes: C15-C26.
Complications of colon adenocarcinoma
Complications of adenocarcinoma usually develop at advanced stages of the oncological process, but there are cases that they are the first signs of the disease:
- Intestinal obstruction. It can be compensated, subcompensated and decompensated. Decompensated intestinal obstruction (complete obstruction) is observed in the final sections of the colon, most often at the level of the sigmoid or rectum, since in these places the intestinal lumen is narrower than in the higher sections, and the intestinal contents have a dense structure. In any case, intestinal obstruction requires surgical treatment. Previously, a colostomy was performed for this purpose - the overlying part of the intestine is brought out onto the stomach. Now preference is given to resection of the intestinal section along with the tumor, with anastomosis. If this is not possible, then they resort to ostomy.
- Perforation of the intestinal wall. A very serious complication, since it contributes to the release of intestinal contents into the abdominal cavity or retroperitoneal space with the development of severe peritonitis.
- Inflammatory processes in the tumor. Perifocal inflammation is more common, intratumoral inflammation is less common. Inflammation is associated with the presence of pathogenic microflora in the intestinal lumen, which infects the tumor. The danger of such processes lies in the formation of infiltrates, phlegmon, abscesses, as well as perforation of the intestinal wall and the development of peritonitis.
- Bleeding. Chronic blood loss leads to the development of iron deficiency anemia and, as a consequence, to a decrease in hemoglobin, general weakness, and dizziness. The clinical picture will be determined by the location of the tumor. With severe bleeding of the tumor in the overlying sections, black stools are observed. If a tumor of the terminal sections of the large intestine bleeds, scarlet blood or blood clots are found in the stool. Many patients mistake them for manifestations of hemorrhoids.
- Tumor growth into neighboring organs, accompanied by disruption of their functioning. For example, when a tumor grows into the liver, symptoms of cholecystitis may develop. If adenocarcinoma of the colon grows into hollow organs, fistulas occur.
Complications
Despite the fact that the tumor itself is a serious disease, it can also cause other complications, which include:
- intestinal obstruction caused by a tumor that grows into the lumen of the organ is diagnosed in 40% of patients;
- perforation (rupture) of the walls of the organ - causes profuse internal hemorrhage;
- formation of ulcerations on the surface of a cancerous tumor;
- the occurrence of interorgan fistulas, as well as the development of peritonitis;
- intussusception - when one part of the intestine invades another;
- in the case of left-sided lesions, a change in the shape of feces (sheep feces) is possible.
Existing complications significantly complicate the treatment process and worsen the patient’s condition.
Forecast
Mainly, the prognosis of adenocarcinoma depends on the histological type of the tumor and the stage of the disease at the time of treatment. The most favorable situation is in the initial stages, when there are no regional or distant metastases yet. The five-year survival rate of such patients is 95% for the first stage and 75% for the second stage (all types of tumors are taken into account, even the most malignant ones). Only half of the patients survive the five-year mark in the third stage, and about 5% in the fourth stage.
Thus, the sooner treatment is started, the more favorable the prognosis will be. The European Oncology Clinic provides treatment for colon adenocarcinoma at all stages of the disease, including terminal ones. If a cure is not possible, we focus our efforts on improving the quality of life of patients.
Book a consultation 24 hours a day
+7+7+78
Nutrition
During treatment, patients are prescribed dietary nutrition. A balanced diet strengthens the immune system. The body needs strength to heal. Taking into account the patient’s health condition and the stage of oncology, the diet is compiled individually. The menu is formed taking into account the following principles:
- reduced calorie content;
- limiting animal fats;
- limiting foods rich in calcium;
- inclusion in the diet of substances that stop the onset of cancer.
The diet limits the content of red meats (pork, beef, etc.) to 70 grams. per day. Meat is replaced with fish and poultry. The daily diet includes fresh vegetables, fruits and herbs. Low-fat fermented milk products are beneficial, including kefir, fermented baked milk and organic yogurt.
Diagnosis of the disease
Diagnosis of adenocarcinoma of the cecum begins with an external examination of the patient; the doctor should pay attention to the color of the person’s skin and mucous membranes.
He also palpates the abdomen to determine the presence of tumors in the intestines and liver. They prescribe a general blood and stool test for hidden blood in it.
Next, the urologist or gynecologist conducts a digital examination of the rectum and vagina in women. It will help determine the presence of a neoplasm, its approximate location, as well as the condition of the rectum, ovarian uterus and vaginal wall, which may also be involved in the tumor process.
To confirm the diagnosis, the following methods are used:
- rectoscopy (examination of the rectum and sigmoid colon using an endoscope inserted through the anus). An accurate method that will allow you to see adenocarcinoma in these parts of the large intestine. Rectoscopy is often used for preventive purposes. But the endoscope does not allow access to the cecum. Therefore, other methods are used;
- colonoscopy. The essence is the same as that of rectoscopy, but this technique allows you to examine the entire large intestine. During this procedure, a piece of tumor tissue may be taken for examination in the laboratory. This procedure is called a biopsy. It is necessary to determine the type of cancer and determine further treatment;
- irrigoscopy. The x-ray method involves the introduction of a contrast agent, which is distributed in the intestines and then viewed on an x-ray. In this way, you can see the contours of the organ and possible defects and complications, but minor deviations cannot be detected using irrigoscopy. Other radiological methods are also used that make it possible to identify metastases in other organs (chest radiography, urography, cystography, urethrography and others);
- More accurate imaging methods include ultrasound of the pelvic and abdominal organs. It shows possible lesions in the intestine and neighboring organs, as well as the depth of tumor infiltration. Ultrasound is a painless and inexpensive method;
- CT and MRI. They provide even more information than ultrasound and show even the smallest defects. They may be prescribed if the results of other studies are unclear.
Based on the results obtained, the doctor can prescribe treatment.
Diagnostics
Doctors are able to make a diagnosis of intestinal oncology by studying the medical history, complaints, organizing an examination, digital diagnostics and instrumental examination.
Important! 60% of all tumor cases are located in the lower colon, which makes it possible to detect them through a digital examination or sigmoidoscopy.
When a malignant neoplasm is located at the top of the intestine, it can only be diagnosed using a colonoscopy. During an examination with an endoscope, a specialist obtains a tumor sample from the intestine for morphological laboratory testing.
To assess the prevalence and size of adenocarcinoma, radiographic diagnosis is required. To establish the presence of metastases and contraindications to endoscopy, an ultrasound scan of the abdominal and pelvic organs is first performed.
Ultrasound
In difficult cases, the patient is referred to a CT or MRI of the abdominal region. A general blood, urine, and stool test is required. The final diagnosis is made after a biopsy of a sample of tumor tissue.
Causes and characteristics of the pathology
Moderately differentiated adenocarcinoma can reach a large size, because rapid spread of cancer cells occurs. This disease of the colon causes intestinal obstruction, wall rupture, and bleeding. It can be complicated by peritonitis and the occurrence of fistula tracts. There is a high probability of transition to a low-differentiated stage. After tumor removal, five-year survival is observed in 75% of patients.
The reasons for the development of the disease have not been fully established. The development of a malignant cancer tumor is provoked by the following reasons:
- work activities associated with hazardous substances;
- genetic predisposition;
- colon diseases;
- constant interaction with household chemicals;
- bad habits;
- intestinal diseases;
- frequent stressful conditions;
- excessive consumption of fatty foods and salt.
The development and spread of cancer cells is often influenced by several factors simultaneously.