Rectal cancer is one of the tumors for which a simple examination is sufficient to diagnose; unlike other colon tumors, it is sensitive to radiation and chemotherapy, but the best result is achieved only when they are combined with surgery. Typically, the tumor occurs in the middle section of the intestine, called the ampulla.
Our expert in this field:
Ryabov Konstantin Yurievich
Chief surgeon, oncologist, endoscopist
Call the doctor
Causes of rectal cancer
The main risk factor is polyps, but not all of them, but those with a villous structure. In addition, the likelihood of a polyp becoming malignant is related to its size and duration of existence; the larger the size, the higher the likelihood of cancer, so all polyps must be removed.
Adenocarcinoma develops more often in East Asian peoples and is believed to be closely related to dietary habits and genetics. For some reason, the disease is more common in men, but heredity does not play a significant role.
Diagnosis of rectal cancer
Rectal cancer is recognized as a disease that can be detected very early - this is the visual localization of a malignant tumor. To detect pathology of the rectum, complex devices are not required; the surgeon only needs to feel the inside of the intestine with his finger. Digital examination is included in the standard surgical procedure, but is performed very rarely, so the disease is rarely detected at an early stage.
Cancer reveals itself with unpleasant symptoms, usually a change in the character of stool, pain and bleeding, but at the beginning of the development of a malignant neoplasm, no clinical signs are observed.
Classification
Tumors are classified according to the type of cell division, origin, and shape. Based on the first sign, the process is divided into 2 large categories:
- benign;
- malignant.
Benign tumors of the rectum can be epithelial or nonepithelial, carcinoids. The first include polyps, polyposis, the second - fibroma, lipoma, fibroids. A separate category is carcinoid, which is a tumor associated with hormone levels.
Malignant neoplasm of the rectum may also be associated or not associated with the epithelium. The first are adenocarcinoma, melanoma, the second are rhabdomyoma, angiosarcoma.
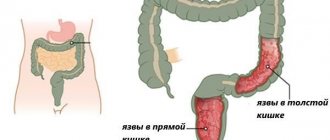
Rectal cancer is divided into several categories based on location: supraampullary, ampullary, anal. The first type is a high location; with this form, the lumen of the cavity quickly narrows. Stenosis increases, in which feces cannot pass through the intestines as needed.
When an ampullary part of the intestine is formed, the tumor either swells, protruding into the organ, or may have the appearance of a bleeding crater. The last form listed is located in the anal area; its structure is often squamous cell carcinoma.
Based on the relationship of malignant cells to the organ wall, exo-, endophytic, and mixed forms of neoplasms are distinguished.
Cancer is classified according to its histological structure:
- squamous;
- slimy;
- solid;
- fibrous;
- undifferentiated.
This classification is related to the type of cells in which the growth disorder begins.
Benign tumors
Benign tumors of the rectum differ in types and can be in the form of:
- polyp;
- villous formation;
- vascular defect;
- polyposis;
- fibroids, lipomas, fibromas;
- cavernous type angiomas.
A polyp is a growth of the mucous membrane, formed from epithelial type cells. It can have different shapes, sizes, and be localized throughout the intestine. The growth begins to cause symptoms only when the stalk becomes long. If it has a wide base, then there may be no pain at all.
Polyposis is a multiple formation, the elements are located in groups. This form of benign process is genetically determined. It occurs more often in children and adolescents. There is a form of disorder similar to this disease, but it is associated with intestinal inflammation, pseudopolyposis.
Fibroma is formed from connective tissue; the signs of a tumor may correspond to a malignant form. These are mucous and bloody discharge, constipation, disruption of the sphincter, signs of inflammation of the rectum.
Myoma is a hard polyp, rare, formed from smooth fibers. Lipoma is a soft lobular formation. It is even less common than the previous type, and almost never degenerates into a malignant tumor.
We recommend reading Moderately differentiated adenocarcinomas, their types and treatment
Malignant tumors
A malignant tumor of the rectum is characterized by rapid, uncontrolled growth; only a tumor of this type is capable of growing into neighboring organs and being transferred through the bloodstream to other structures. Cancer can occur due to an untreated benign process.
Different types of malignant process differ from each other in the degree of malignancy and time of manifestation. Adenocarcinoma does not manifest itself in the early stages and is formed from the mucous membrane. It is called a glandular tumor, and treatment depends on the degree of differentiation. It can reach large sizes, blocking the entire lumen of the structure.
Rectal blastoma may or may not be benign. In the first option, it shifts structures located nearby, in the second, it grows through them.
The squamous cell form of cancer spreads quickly and switches to immune organs. Metastases appear in the lymph nodes, bladder, vagina or prostate.
In patients with this type of cancer, symptoms begin soon after the tumor begins to develop. It has a high degree of malignancy and often recurs.
Stages of rectal cancer
Previously, the stages of cancer were determined by the size of the tumor, but it turned out that the depth of penetration of cancer cells into the organ wall and metastases in nearby lymph nodes are much more important for the prognosis, and therefore the choice of optimal treatment. If the tumor does not involve the lymph nodes in the process, then this is early stage I and II cancer.
- In stage I, the tumor is limited to the rectal mucosa.
- Its germination through the entire intestinal wall, but without leaving the organ, transfers the process to stage II.
- Metastases in the lymph nodes near the intestine, regardless of the size of the primary tumor, change the stage to III.
- And stage IV is diagnosed only with metastases in other organs, most often the liver and lungs.
A very important prognostic sign is the degree of malignancy of the neoplasm, which is determined by cell maturity. The more primitive a cell is, the more aggressively it multiplies; cancer from the most primitive cells is called undifferentiated, and it quickly metastasizes. Highly differentiated neoplasms have the lowest malignancy and the best prognosis. Accordingly, moderately differentiated cancer has an average degree of aggressiveness.
Take care of yourself. Make an appointment with an oncologist today
Classification and stages of cancer
Various cancer classification systems are now widely used. The most significant:
- TMN;
- Dukes.
The following designations are accepted in the TMN system:
- Tis is a non-invasive cancer. Atypical cells appeared on the surface layer of the epithelium.
- T1 – tumor less than 1/3 of the circumference and length of the rectum, not affecting the muscle layer of the intestinal wall.
- T2 – the size of the tumor does not exceed 1/2 of the circumference and length of the rectum, infiltrates the muscle layer, and does not cause restrictions on the displacement of the rectum.
- T3 – a tumor measuring more than half the length or circumference of the rectum, causes restrictions in displacement, but has not spread to neighboring organs.
- T4 – the tumor affects neighboring structures.
- N0 – regional lymph nodes without changes;
- N1 – there are metastases to regional lymph nodes. In intestinal cancer, the presence of metastases is determined using lymphography.
- M0 – no distant metastases (in other organs);
- M1 – there are distant metastases.
Dukes classification:
- A – only the mucous membrane is affected by the tumor;
- B – germination of the intestinal wall, regional lymph nodes without changes, no distant metastases.
- C – the tumor has grown through all layers of the intestinal wall, there are regional metastases;
- D – distant metastases were detected.
Classification of cancer by stages
| Stage | TMN | Dukes | ||
| Тis | N0 | M0 | ||
| 1 | T1 | N0 | M0 | A |
| 2 | T2 | N0 | M0 | A |
| 3 | T3 | N0 | M0 | IN |
| 4 | any T | N1-2 | M0 | WITH |
| 4 | any T | any N | M1 | D |
If we evaluate cancer by stages, then:
- 1 – the tumor or ulcer is small, clearly demarcated, located in a small area of the mucous membrane, changes do not affect the muscular layer of the intestinal wall.
- 2 – the tumor does not exceed half the length or circumference of the rectum in size, does not grow into adjacent tissues, and there are no more than 1 regional metastases.
- 3 – the tumor is larger than the semicircle of the intestine, pathological changes affect neighboring organs, there are multiple metastases in regional lymph nodes.
- 4 – the tumor is extensive, disintegrating, or a tumor of any size, but there are distant metastases.
This division into stages is necessary in order to choose a treatment method and predict the approximate life expectancy.
It is impossible to determine not only the stage of cancer, but also the fact that discomfort is caused by this disease, based on clinical symptoms. You definitely need to get tested.
Be sure to read:
Preparation and performance of sigmoidoscopy
Symptoms of rectal cancer in the early stages
The main function of the rectum is the formation and removal of feces. Therefore, the first symptoms of rectal cancer are bowel problems. This may be constipation or diarrhea; at first the symptoms are transient, but as the tumor grows, stools of normal consistency become very rare.
False urges are often a concern , when, with a small amount of feces, an irresistible desire to evacuate occurs, which is called “rectal spitting.” Very often, after a bowel movement there is no feeling of complete bowel movement ; if the cancer is located near the anus, then pain occurs during bowel movements.
The second sign is the appearance of blood in the stool , at first only in streaks, then clots are released, which may be mixed with mucus. The presence of mucus without blood is not considered a sign of colorectal cancer. In case of chronic blood loss, a blood test determines a lack of red blood cells and hemoglobin - anemia .
Intense chronic pain occurs when the entire wall of the organ grows and the pelvic nerve plexus is involved. If the cancer spreads to the bladder, then symptoms of cystitis resistant to standard treatment . When it grows into the vaginal tissue, pain appears during sexual intercourse .
Rectal cancer progresses aggressively even with a favorable histological structure - well-differentiated adenocarcinoma. The process is prone to relapse and rapid metastasis, most often to the liver and lungs. A high degree of malignancy coincides with sensitivity to radiation and chemotherapy, but cancer cells quite quickly develop a self-defense strategy - resistance. The leading method of treatment is surgery, which is preceded by radiation therapy (RT), sometimes together with several courses of chemotherapy (CT), and prophylactic drug treatment is excluded only in stage I.
It is assumed that radical treatment should alone ensure unconditional recovery, but for rectal adenocarcinoma, surgery alone cannot cure the disease . Cancer of this part of the large intestine is treated comprehensively, that is, using all methods: surgery, radiation and antitumor drugs.
The main set of therapeutic measures can be supplemented with innovative local methods of destruction, various physical factors and targeted drugs. But with a widespread process, the most modern approach does not promise a complete cure, which is why it is so important to identify the malignant process at the very beginning, preferably at the stage of a villous polyp.
Causes
Malignant and benign tumors located in the rectum are formed under the influence of approximately the same factors:
- presence of illness in close relatives;
- nature of work;
- bad habits;
- one-sided nature of nutrition;
- other intestinal diseases;
- excess weight;
- hypovitaminosis;
- age over 60 years;
- immunosuppressive conditions;
- constipation.
If a malignant process was observed in parents or in another generation, then the person is at risk for oncology. Working in a workshop with harmful emissions, the nature of activities with heavy metals, toxic gases also contribute to the development of abnormal phenomena.
A tumor in the rectum can form if a person drinks or smokes, especially in cases where the quality of the product is low. Cigarettes contain dozens of carcinogenic substances, which has been confirmed by research. Alcohol is transformed in the liver, but passes through the entire digestive tract. It disrupts the activity of the enzymatic system, dulls the reaction rate, poisons the brain, and damages sensitive cells.
Human nutrition must contain the main groups of substances, for which the diet is made up of vegetables and fruits, cereals, meat and dairy products. From each of these categories the body draws a source of energy. In addition, plant foods are a source of fiber, which has a soluble and insoluble part, due to which the digestive tract is “cleansed” of excess. If a person does not eat vegetables and fruits, the intestines become filled with waste, the excess is not excreted, which damages its walls. Tumors of the rectum and other parts become the result of this process.
Chronic constipation, which occurs due to a malignant process, is associated with a predominance of meat in the diet, especially pork and beef.
A healthy organ that receives a balanced diet cannot get sick. The presence of damage in the form of anal fissures and hemorrhoids, as well as colitis (inflammation of the mucous membrane) are favorable conditions for cell transformation.
Crohn's disease is a precancerous disease that combines several symptoms. It affects the small intestine and the beginning of the large intestine, but affects all parts of the structure. The essence of chronic inflammation is the presence of inflammation of the small or large intestine, which penetrates into the deep layers of the wall, forming ulcers. Leukocytes accumulate around the erosions, forming infiltrates. When the elements heal, rough scars form. Cancer cells can divide in this tissue.
We recommend reading Tumors of the sigmoid colon, their symptoms, causes and treatment
Antioxidants are designed to neutralize substances that cause cancer. If they enter the body in short supply, the protection is weakened. With a sedentary lifestyle and obesity, the risk of tumor increases.
The occurrence of rectal oncology is influenced by a decrease in immunity; it develops due to a deficiency in the synthesis of lymphocytes and natural killer cells, which are responsible for the fight against tumor cells.
Treatment tactics
The tumor is detected by examination with a finger; an endoscopic examination is required - sigmoidoscopy, during which a piece of the tumor is taken for microscopy. A colonoscopy is always performed because it is rare but possible for multiple cancerous nodes to develop in the colon.
Before starting treatment, an MRI of the pelvis is performed, where the size of the formation and the involvement of neighboring organs and pelvic tissue are determined.
Radical treatment of rectal cancer necessarily includes surgery. At stage 1, endoscopic surgery or the most gentle and organ-preserving resection is performed.
The extent of intervention at stage 2 depends on the location of the tumor in the organ and its true size; poorly differentiated adenocarcinoma requires chemotherapy. At stage 3 after surgery, courses of preventive chemotherapy are mandatory and are supplemented with radiation.
For inoperable rectal cancer, photodynamic therapy , which improves the penetration of chemotherapy drugs into the tumor and increases efficiency.
Symptoms
Despite the fact that there are screening methods of examination and the rectum is accessible for visual examination, rectal cancer is detected in the last stages in 30% of patients. This is due to the fact that patients do not attach importance to the first signals of a developing disease.
In the initial stages, the disease is practically asymptomatic; the main signs of cancer appear periodically. As the disease progresses, they intensify and new symptoms appear.
First symptoms
A characteristic sign of the initial stages of the appearance of a neoplasm is pathological discharge. Found in stool:
- Blood. It appears in the form of veins and mucus, usually dark in color, but can also be scarlet. In the first stages, blood in the stool appears periodically (2-3 weeks of bowel movements may be normal, then several days with blood, and again a period of visible well-being begins). With ampullary cancer, blood accumulates in the ampulla of the rectum and flows out during bowel movements before feces.
- Slime. Due to the resulting neoplasm, proctitis develops, which increases the secretion of mucus. It is found along with bloody or purulent discharge. Sometimes an admixture of mucus is released along with feces in the form of small clusters of translucent whitish flakes.
Early signs of cancer are symptoms of impaired intestinal function:
- Constipation. Cancer is characterized by the fact that feces, after a long delay in stool, are excreted profusely and have a foul odor. Patients often complain of a feeling of incomplete bowel movement after defecation, leading to false urges. Obstruction is typical for tumors located in the rectosigmoid region.
- Diarrhea. Persistent diarrhea, unresponsive to medication, occurs due to the development of proctitis and is associated with excessive production of intestinal mucus. “False” diarrhea occurs (with frequent urges, a small amount of mucus and bloody masses are released).
- Alternating constipation and diarrhea. This symptom occurs against the background of partial intestinal obstruction. The rhythm of bowel movements is inconsistent.
- Change in the shape of the stool column. With rectal cancer, symptoms rarely appear. Fecal masses are flattened, in the form of balls, strands, threads. Although this symptom is more typical for spastic colitis, if the symptom appears systematically, it is imperative to be tested for cancer.
Since the rectum is divided into 3 anatomically different sections, the symptoms of cancer depend on the location of the tumor.
Anorectal cancer is characterized by:
- spread beyond the mucous membrane of the anal canal;
- violations of the act of defecation;
- discharge of blood, mucus, pus from an ulcer or fistula around the anus;
- impaired urination (if the urethra is involved in the tumor process).
With ampullary cancer, the tumor does not appear for a long time. When it becomes significant in size, the feces injure it, and then the following occurs:
- bleeding during or after defecation;
- frequent, painful urges.
Supramullary manifests itself:
- frequent constipation, occasionally alternating with diarrhea;
- pain in the anus that intensifies with defecation or walking.
Such symptoms are also characteristic of benign diseases of the rectum. Patients often simply do not pay attention to the first signs of a dangerous disease, especially if they previously had colitis, proctitis, or hemorrhoids. They begin to take medications that eliminate symptoms (this makes early diagnosis of cancer difficult), and use anti-hemorrhoid suppositories. Sometimes, they are simply embarrassed to see a doctor, because the symptoms appear periodically and are easily explained. And pain in the early stages is often absent. Meanwhile, the tumor is growing. The patient's condition worsens.
Further development of symptoms
If the tumor is exophytic (grows into the intestinal lumen), it rarely grows into the thickness of the wall, and does not bother the patient for a long time until mechanical obstruction occurs or the tumor “falls out” of the anus. By this time, it is already capable of metastasis.
An endophytic tumor quickly grows through the wall of the rectum, reaches the peritoneum, the tissue surrounding the ampullary and anorectal parts of the rectum, and spreads to the adjacent pelvic organs.
As the pathology progresses, the main symptoms intensify:
- Pathological discharge. In the later stages, due to the disintegration of the tumor and the addition of infection, in addition to mucous and bloody discharge, impurities of pus are found in the stool. With ordinary inflammations, the pus is usually whitish and greenish, and with cancer it is yellowish and brown.
- Pain. With ampullary cancer, pain appears when the tumor grows through the entire thickness of the intestinal wall. Painful sensations are associated with tumor growth into adjacent tissues and compression of nerve fibers. Often, when this symptom appears, patients are diagnosed with advanced tumors. The exception is malignant neoplasms of the lower ampullary region and anus. With cancer of these sections, pain appears early, it is burning, patients complain that it intensifies not only during bowel movements, but also interferes with sitting.
Be sure to read: Intestinal dolichocolon in adults: definition of pathology and treatment
Rectal cancer is characterized by a late appearance of general symptoms:
- anemia;
- weakness;
- weight loss;
- irritability;
- earthy skin tone.
As the tumor grows, patients complain of pain in the coccyx, lower back, and sacrum. Performance is significantly reduced due to frequent false urges at night, and insomnia occurs.
Untimely or late access to a doctor leads to the tumor metastasizing. Secondary lesions occur in any organ. Most often, rectal cancer metastases affect:
- liver;
- lungs;
- brain, spinal cord;
- adrenal glands;
- bones.
The main danger of cancer is precisely that they occur with minor clinical manifestations, and only in the last stages does pain and intensification of other leading signs force the patient to seek medical help.
What operations are performed for rectal cancer?
- For early adenocarcinoma, organ-preserving endoscopic transanal resection , when the entire malignant tumor is removed microsurgically layer by layer with a small section of the intestinal wall. The cancerous lesion must be very small in size - no more than 3 cm and occupy no more than a third of the circumference of the intestine, not penetrate beyond the mucous membrane and without signs of cell aggressiveness. If, with a minimal operation, subsequent histological examination reveals unfavorable prognostic signs, a repeat operation of a larger volume is possible.
- During mesorectumectomy , a fairly large part of the organ is excised; depending on the location of the cancer conglomerate, this resection option can be partial or total, without temporary removal of the end section to the abdominal wall and with an ileostomy. In the lower third of the intestine, closer to the anus, an almost similar intervention option is called abdominal-anal or intersphincteric resection. If it is necessary to remove the anus onto the stomach, after some time the patency of the intestinal tube is completely restored, as a rule, after completion of preventive chemotherapy.
- Today, mutilating abdominoperineal extirpation , when the cancerous lesion does not allow another option; large amounts of tissue are removed in the process of evisceration of the pelvis in case of relapse after radical treatment. In both cases, the intestine is exposed to the abdominal wall - an unnatural anus is created, and a postoperative scar remains in place of the anatomical anus.
Today they try to perform surgery on every patient. If the tumor is not initially operable, then at the first stage chemoradiotherapy is performed, after which the possibility of delayed surgical treatment is discussed. As a rule, the likelihood of surgical intervention is doubtful in case of multiple and non-removable metastases, but the patient is required to be consulted by an oncologist surgeon, more than once and at all stages of treatment.
Reviews from our patients
- Mammary cancer. Full recovery
Mammary cancer. Full recovery February 19, 2021Here is a case of complete recovery from breast cancer. Two weeks ago, a patient came to us with a complaint of a tumor in the right mammary gland. A biopsy was performed. Based on its results, cancer was diagnosed. The tumor is highly differentiated, susceptible to the influence of hormones. A surgical operation for resection of the mammary gland was performed. The breast is preserved. According to the results of histological examination, the surgical intervention was carried out radically, the resection margins were clean. To prevent…
read more
- Treatment at the Medicine clinic 24/7. Patient review
Treatment at the Medicine clinic 24/7. Patient review February 16, 2021
The patient underwent examination and chemotherapy treatment. He notes: “I would like, first of all, to express my gratitude. Secondly, the impression of the clinic and the attending physician as the highest professionals. Extreme level of competence, efficiency, organization and interconnectedness of decision making. All this leads to a positive result. Therefore, I want to express my gratitude to all of you for all this. I didn’t even expect that such a level of service in medicine was possible......
read more
- Preparing for chemotherapy: Increasing hemoglobin levels
Preparing for chemotherapy: Increasing hemoglobin levels February 11, 2021
The patient was admitted to the clinic with a low hemoglobin level. This factor interferes with chemotherapy. In other medical institutions it may be a reason for refusal of treatment. In such situations, specialists at the Medicine 24/7 clinic carry out a set of measures aimed at increasing hemoglobin levels. We have a similar case before us. During hospitalization, blood counts returned to normal. The patient was discharged with improved health.
read more
- Treatment of pleurisy: patient review
Treatment of pleurisy: patient review February 11, 2021
The patient came to the Medicine 24/7 clinic due to pleurisy, which acutely arose against the background of the underlying disease. Treatment was carried out promptly. Fluid from the pleural cavity was evacuated. Specific treatment of the underlying disease was started. The patient thanks her attending physician for the assistance provided. She notes his attentiveness and kindness.
read more
- Photodynamic therapy: patient review
Carrying out photodynamic therapy: patient review February 10, 2021
The patient applied to the Medicine 24/7 clinic for treatment of skin basal cell carcinoma. Treatment was prescribed in the amount of photodynamic therapy. A positive result has been achieved. During a comprehensive examination, kidney disease was revealed. Treatment tactics have been developed. Patient o.
read more
- Chemotherapy: patient review
Chemotherapy: patient review February 10, 2021
The patient was hospitalized for a second course of chemotherapy. Her condition remained serious. During hospitalization, the patient was prepared for treatment. A course of antibacterial therapy was carried out. Bilateral pneumonia was stopped, as well as bleeding. The patient successfully completed the second course of chemotherapy. The treatment prognosis is favorable.
read more
- Treatment of stage 3 ovarian cancer with peritoneal carcinomatosis
Treatment of stage 3 ovarian cancer with peritoneal carcinomatosis February 5, 2021
The patient came to the clinic due to stage 3 ovarian disease. A comprehensive examination was carried out. The diagnosis is confirmed. The situation was discussed at a medical council, the decision of which proposed cytoreductive surgery and the HIPEC procedure. The surgery was successful. On the seventh day after surgery, the patient was discharged home in satisfactory condition. In the future, it is planned to conduct six courses of chemotherapy, the goal of which is to avoid relapse.
read more
How are stages 1, 2 and 3 rectal adenocarcinoma treated?
For early stage 1 cancer , endoscopic resection is used; most patients are cured without any additional effects, so neither radiation nor chemotherapy is performed.
In case of greater damage to the thickness of the intestinal wall by a malignant process, but without screening out cancer cells in the peripheral lymph nodes - stage 2, a section of the organ is also resected, but this time extensively - with mesorectumectomy. If the likelihood of relapse is low, treatment is considered complete. If there are cellular signs of an unfavorable prognosis, preventive chemotherapy is carried out for six months.
For stage 3 adenocarcinoma, radiation is performed before surgery. With 5-day radiation therapy with large fractions, resection is performed already on the 3rd day after the last session, but in very elderly patients or with concomitant chronic diseases, the intervention can be postponed for a month and a half until full recovery.
With long-term 10-12-week irradiation against the background of weekly drug injections (to improve the result), the operation is performed one and a half to two months after the completion of radiation therapy sessions. When radiation therapy is not given before surgery, it is given after surgery to prevent early cancer recurrence. All patients are required to undergo preventive chemotherapy for six months.
What tactics are adopted for stage 4 cancer?
In case of an initially inoperable stage 3 process - a large neoplasm embedded in the surrounding tissues - at the first stage, long-term radiation therapy is carried out along with drug therapy. If the tumor has decreased and technically the intestine can be removed, then the operation is planned in 10-12 weeks, and chemotherapy courses are carried out before it. If after long-term irradiation it is not possible to remove the adenocarcinoma, several more courses of chemotherapy are performed - 4-6, after which they return to discussing the possibility of removal. After surgery, chemotherapy exposure is increased to a total duration of six months.
Stage 4 is not a contraindication for surgery if metastases in the liver and lungs can be removed, but at the first stage up to 6 courses of chemotherapy are done. After chemotherapy, surgery is performed with simultaneous excision of the rectal tumor and resection of metastases, or all tumors are removed in several approaches, including such innovative methods as laser or radiofrequency ablation (RFA), cryodestruction.
If multiple metastatic foci cannot be removed, palliative intestinal resection is not excluded, again against the background of systemic multi-course drug treatment. There are many options for combining methods, but surgical intervention is always a priority.
Get a comprehensive treatment plan
Treatment
The treatment tactics for benign and malignant neoplasms in the rectum will be slightly different.
In the first case, the basis of treatment is:
- surgery to remove the tumor - complete resection of the lesion;
- minimally invasive procedures, in particular electrocoagulation;
- Medication methods are individual for each patient.
As for cancer, a malignant tumor of the rectum is treated using the following methods:
- chemotherapy - both before and after surgery;
- radiation therapy;
- surgical removal of a rectal tumor simultaneously with affected lymph nodes and malignant areas of other internal organs.
Medical intervention can be performed in one of the following ways:
- resection of a separate part of the rectum or anal sphincter;
- abdominal-anal resection;
- abdominoperineal extirpation;
- pelvic evisceration;
- amputation of the rectum.
All patients with this diagnosis are advised to follow a gentle diet. In cases of benign or malignant lesions of the rectum, the diet will have the following rules:
- consuming sufficient amounts of proteins, fats, carbohydrates, minerals and vitamins;
- minimizing the consumption of fatty meat dishes;
- enriching the menu with fresh or steamed vegetables and fruits;
- compulsory full breakfast;
- fractional consumption of food - 5 times a day;
- thoroughly chewing food components;
- complete rejection of hot and sour foods;
- food temperature control;
- drinking enough liquid.
A list of permitted and prohibited foods, recommendations for food preparation and a sample menu will be provided by your attending physician.
It is not advisable to use other methods of therapy, including traditional medicine, since self-medication can only aggravate the situation.
What chemotherapy is used for rectal adenocarcinoma?
- For adjuvant or preventive chemotherapy, FOLFOX and XELOX regimens are provided.
- At stages 2 and 3, only tablet forms of drugs are used. The duration of prophylaxis is 6 months.
- for the treatment of generalized metastatic process . A unified strategy has not been developed, the following options are possible: do a six-month course of chemotherapy until the cancer process stabilizes and stop without resorting to chemotherapy until signs of progression appear; after 3-4 months of combination chemotherapy using any of the regimens, continue treatment to maintain the achieved result; The third approach is to treat while there is no severe toxicity or there is enough strength.