Classification of small bowel cancer
There are five types of malignant tumors found in the small intestine:
- Adenocarcinoma is, strictly speaking, only cancer. These tumors develop from glandular cells of the mucous membrane, most often found in the jejunum and duodenum.
- Sarcoma is a malignant tumor of connective tissue. The most common tumors are leiomyosarcomas , which are smooth muscle tumors in the intestinal wall. These tumors usually affect the ileum. Gastrointestinal stromal tumors originate from Cajal cells , which are located in the walls of the digestive tract from the esophagus to the anus and provide motility - smooth muscle contractions.
- Carcinoid tumors belong to the group of neuroendocrine tumors . They are most often found in the ileum.
- Lymphomas are tumors of lymphoid tissue. Non-Hodgkin's lymphomas most often occur in the small intestine , usually in the jejunum and ileum.
Treatment
Treatment of a malignant tumor in the small intestine depends on the degree of damage to the organ and the type of oncology. In approximately 2/3 of all cases, surgery is performed to remove cancer cells. This helps reduce the intensity of symptoms and increase the patient's life expectancy.
Important! Sometimes the operation has only palliative value, that is, it is performed with the sole purpose of alleviating the patient’s suffering.
When the operation is impossible or the tumor formation is sensitive to the effects of chemotherapy, it is performed. Chemotherapy drugs inhibit the growth of cancer cells, preventing them from multiplying and developing normally.
Radiation therapy is ineffective for small intestinal cancer, which is why it is not performed. This can take place immediately after or during surgery to improve positive results. Radiation therapy is also used when surgery is impossible for some reason.
After surgery is completed, the patient is advised to undergo rehabilitation to eliminate the symptoms of cancer and try to completely get rid of cancer cells. Your doctor may prescribe the following medications:
Chemotherapy
At the same time, radiation therapy is implemented. But all of the above procedures can cause a large number of side effects:
- poor health and weakness,
- nausea with vomiting,
- diarrhea,
- constant headaches,
- hair loss,
- disruption of hematopoietic processes,
- mouth ulcers,
- dysfunctions of the immune system.
Due to the fact that the patient’s body is difficult to tolerate treatment, he requires the organization of adequate nutrition, which presupposes compliance with the following conditions:
Rejection of bad habits
Important! In severe stages of the pathology, when surgery is not practical, only radiation and chemotherapy are performed to relieve pain and other severe manifestations of oncology.
Causes and risk factors for small intestine cancer
The causes of the disease are unknown: it is impossible to say exactly what exactly led to mutations in the cell and its malignant degeneration in each specific case. The only known factors that increase the risk of the disease are:
- A high-fat, low-fiber diet.
- Crohn's disease , a chronic inflammatory bowel disease, increases the risk of small bowel cancer by about 6 times.
- Celiac disease is a disease in which the villi of the small intestine are damaged and a person cannot tolerate gluten , a protein found in many grains.
- Familial adenomatous polyposis is a hereditary disease in which there are hundreds or thousands of polyps in the large intestine. Over time, these polyps are highly likely to transform into a malignant tumor; in addition, the risk of cancer of the duodenum, stomach, thyroid gland, liver ( hepatoblastoma ), and pancreas increases.
Book a consultation around the clock +7+7+78
Symptoms of small intestine cancer
Often the tumor does not cause any symptoms. But even if symptoms are present, they are nonspecific and most often indicate some other disease. You need to visit a doctor and get checked if there is blood in the stool for a long time, or the stool has become dark, black, like tar. Prolonged abdominal pain, diarrhea, unexplained weight loss, severe nausea and vomiting are all possible signs of small bowel cancer. An accurate diagnosis can only be established after examination.
Diagnostics
Diagnosing small intestinal cancer is not an easy task, requiring the doctor to have in-depth knowledge of the course of the pathological process. Diagnosis must be preceded by a correct history taking, indications of previous diseases, as well as a description of the onset of the existing disorder.
Initially, it is necessary to assess the general appearance of the patient, the color of his skin, behavior, and gait. If you are careful, even such minor details can point you in the right direction of your search.
Very often, a tumor can creep in or grow into a vessel, which gradually becomes the cause of the development of anemia.
Anemia is a condition caused by a decrease in the concentration of hemoglobin in the blood. Such patients will have pale skin and mucous membranes, they will feel constant weakness and cannot tolerate physical activity well. To compensate for the reduced level of partial pressure of oxygen, such patients will need to carry out a large number of respiratory movements, which is expressed in the form of shortness of breath.
If you use physical research methods, then upon palpation you can feel a tumor-like formation on the anterior abdominal wall. It is usually painful, has an irregular shape and is heterogeneous in its structure. With the help of palpation, one can only indirectly judge the size and consistency of the tumor, so this method is not specific and will only allow one to suspect the presence of an oncological process.
It is difficult to hear something special by auscultation and can only be achieved in the later stages of the disease. When the tumor reaches a large size and blocks the intestinal lumen, the noise of peristalsis of the digestive tract disappears and the so-called “falling drop” symptom appears. When “tapping”, you can listen to a dullness of percussion noise in the projection above the tumor.
Laboratory research
The diagnostic algorithm for a tumor of the small intestine includes:
- Clinical analysis of blood, urine
- Feces for occult blood
- Blood chemistry
- Tumor markers
- Ultrasound
- X-ray of the abdominal organs with contrast enhancement
- EFGDS
- Colonoscopy and irrigoscopy
- Biopsy and histological examination
- CT scan
- Magnetic resonance imaging
Laboratory research methods include a number of tests that help in diagnosing the disease. It should be said that there are simply no specific tests that speak in favor of the presence or absence of an oncological process. But there are several indicators that allow us to suspect the development of an oncological process.
A general blood test shows us the main indicators, the number of red and white blood cells, as well as their ratio. As mentioned above, anemia often occurs as the tumor grows; in tests, this is manifested by a decrease in hemoglobin concentration, as well as erythrocytopenia. All this speaks in favor of hemorrhagic anemia.
White blood cells can be either increased or decreased, or may even be normal; there is no definite dependence here, since this indicator is not specific to the tumor process.
Changes in the biochemical blood test begin with the development of complications of a tumor of the small intestine. Prolonged vomiting with intestinal obstruction leads to thickening of the blood - the hematocrit increases, changes in ionic ratios occur, and metabolic alkalosis develops in the body - a shift in pH to the alkaline side.
When the tumor obstructs the papilla of the common bile duct, obstructive jaundice develops. In a blood test, this will be manifested by an increase in the concentration of total and bound bilirubin.
When analyzing stool, hidden blood can be detected, which can lead us to the development of an oncological process.
For carcinoma, the detection of tumor markers is most indicative. Tumor markers are special biological compounds that are waste products of a neoplasm or synthesized by healthy tissues of the body as a response to a pathological process.
This indicator allows you to suspect the presence of a tumor and prevent further progression of growth with timely treatment. Tumor markers are a very convenient diagnostic method, especially when you need to examine a large number of people. Small intestinal tumors are characterized by CEA, ACE, CA 19-9, CA 242, CA 72-4, Tu M2-RK.
Diagnosis of small intestine cancer
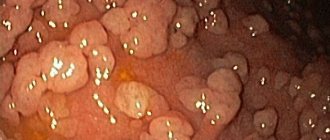
You can examine the duodenum from the inside during fibrogastroduodenoscopy (FGDS) . If the doctor discovers a pathologically changed area on the mucous membrane, he can immediately perform a biopsy and send a piece of tissue for histological and cytological examination.
Special endoscopic techniques are used to examine the jejunum and ileum. During capsule endoscopy, the patient is given a capsule containing a miniature video camera to swallow. It travels through the digestive tract and records an image. With balloon enteroscopy, a tube equipped with one or two balloons is inserted into the small intestine and an endoscope is passed inside it. It can be pulled out of the tube. During balloon enteroscopy, a biopsy can be performed, bleeding can be stopped, and a small tumor can be removed. The end of the small intestine can be examined during a colonoscopy , a test in which a special instrument called a colonoscope is inserted through the anus.
The location of the narrowing in the intestine can be shown by a contrast-enhanced x-ray. Some time before taking x-rays, the patient is given a suspension of barium sulfate to drink. The drug travels through the digestive tract and creates a noticeable shadow in photographs. Sometimes contrast is injected through a probe directly into the duodenum. Barium enemas are used - with the help of such contrast it is sometimes possible to examine the final part of the small intestine.
Computed tomography and MRI are used to assess the location, size and number of tumors, and to identify lesions in the liver, lungs and other organs. To obtain a more informative image, contrast is used: it is administered intravenously or given in tablet form.
PET scanning helps find small metastases that have not been detected by other methods. The patient is injected with radioactively labeled sugar. Since tumor cells need a lot of energy, they absorb this sugar in much greater quantities than healthy tissue. Due to the accumulation of radioactive tracers, tumor foci are clearly visible in images taken using a special apparatus. PET is often combined with CT.
Structure of cancer cells at the histological level
Based on the histological structure, the oncological process of the jejunum is divided into:
- Adenocarcinoma is a fairly rare type of neoplasm. Affecting the duodenum, it is localized in the area of the duodenal papilla.
- Carcinoma is a tumor process that can develop from epithelial cells. It is localized in one of the sections of the colon or jejunum, but is mainly found in the rectum and ileum or appendix.
- Lymphoma – This type of cancer is not common. The main manifestation is lymphogranulomatosis and Hodgkin's disease.
- Leiomyosarcoma - the damage to the organ is so great that it is felt upon palpation through the abdominal wall. Large tumor sizes threaten intestinal obstruction with subsequent rupture of the intestinal walls and bleeding.
Leiomyosarcoma of the intestine
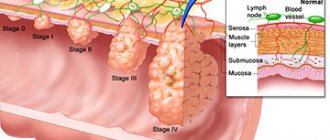
Stages of small intestine cancer
There are five stages of intestinal adenocarcinoma:
- Stage 0 : “cancer in situ.” A single small tumor that is located on the surface of the mucous membrane and does not grow deeper.
- Stage I : The tumor has grown deeply into the intestinal wall, but has not spread to neighboring organs.
- Stage II : the tumor has grown through the entire thickness of the intestinal wall and has spread to neighboring organs.
- Stage III : Cancer cells have spread to regional lymph nodes.
- Stage IV : There are distant metastases. Most often they are found in the lungs and liver.
Stages
The stages of small intestinal cancer are presented using the example of adenocarcinoma. For GI stromal tumors or carcinoids, a different staging system may be used.
| Stage | Grouping by TNM | Description |
| 0 | Tis N0 M0 | Neoplasm only in the epithelium (the upper layer of mucosal cells). It has not grown into the deeper layers of tissue (Tis). No spread to regional lymph nodes (N0) or distant parts of the body (M0). |
| I | T1 or T2 N0 M0 | The neoplasm has grown into the deeper layers (lamina propria or submucosa) (T1), or through the submucosa into the muscularis propria (T2). No spread to regional lymph nodes (N0) or distant parts of the body (M0). |
| IIA | T3 N0 M0 | The neoplasm grew through the muscularis propria into the subserosal layer. No invasion into any adjacent organs or structures (T3). No spread to regional lymph nodes (N0) or distant parts of the body (M0). |
| IIB | T4 N0 M0 | The tumor has grown through the outer layer of tissue lining the intestine (serous or visceral peritoneum) or into adjacent organs or structures (T4). No spread to regional lymph nodes (N0) or distant parts of the body (M0). |
| IIIA | Any T N1 M0 | The neoplasm has grown into any layers of the intestinal wall (Any T). There is spread to 1 or 2 regional lymph nodes (N1) but not to distant parts of the body (M0). |
| IIIB | Any T N2 M0 | The neoplasm could grow into any layers of the intestinal wall (Any T). It has spread to 3 or more regional lymph nodes (N2) but not to distant parts of the body (M0). |
| IV | Any T Any N M1 | The neoplasm can grow into any layers of the intestinal wall (Any T). There may or may not be spread to adjacent lymph nodes (Any N). Spread to distant lymph nodes or organs such as the liver or peritoneum (inner lining of the abdomen) (M1). |
Surgery
Surgeries for small intestine cancer can be radical or palliative . During radical surgery, the surgeon removes the affected area of the intestine, including healthy tissue above and below, and nearby lymph nodes. If the cancer has spread to neighboring organs, they are also removed.
Palliative operations are aimed at improving the patient's condition. If the tumor blocks the intestinal lumen, a bypass anastomosis is performed.
Symptoms
With an exophytically growing tumor, there is a risk of developing intestinal obstruction. Depending on the degree of obstruction of the intestinal lumen by the formation, the clinical picture of the condition will depend. With increasing mechanical obstruction, the patient will be disturbed by the following complaints:
- Abnormal stool. Initially, diarrhea may develop, followed by constipation.
- Pain syndrome. Characterized by a gradual increase in pain intensity, up to sharp paroxysmal colic
- Nausea, belching with fecal odor
- Bloating, distension of the intestines
- Profuse vomiting of intestinal contents, followed by slight relief
- In advanced cases - dilated intestine visible to the naked eye, paroxysmal severe pain, rumbling
With prolonged vomiting, dehydration occurs and symptoms of intoxication appear. If this condition is not treated, peritonitis may develop - a rupture of the intestinal wall with the release of intestinal contents into the abdominal cavity.
There are some differences in symptoms when the tumor is localized in the duodenum.
If small intestinal cancer forms near the papilla of Vater, the clinical picture will resemble duodenal ulcer. In this case, the patient is bothered by pain in the epigastric region. In this case, eating and drug therapy will not bring relief.
If the tumor completely blocks the lumen of the duodenum in the initial part, then the patient complains of distension in the epigastric region, profuse vomiting, after which relief comes. It is noteworthy that bile is not mixed with vomiting, since the common bile duct is located below the site of obstruction.
A tumor that develops in the periampullary portion of the duodenum will be characterized by symptoms of compression of the common bile and Wirsung ducts. Bile from the duct will not be able to enter the intestines, while the gallbladder will gradually fill, then the bile will begin to enter the bloodstream through the vessels in the liver. The skin becomes yellow in color and itching may occur. A biochemical blood test will show an increase in total and direct bilirubin.
Small intestinal cancer localized in the infraampullary part of the duodenum, jejunum and ileum will manifest itself only with the development of mechanical obstruction or with ulceration of the vessel with the development of bleeding.
With endophytically growing malignant neoplasms, the tumor grows through the thickness of the intestinal wall. Further development of the disease can follow several paths:
- Perforation of the intestinal wall with the release of contents into the abdominal cavity leads to the development of peritonitis - inflammation of the peritoneum. This is a life-threatening condition. Only emergency laparotomy will save the patient from death.
- A tumor that grows into the intestinal wall can form a narrowing of the lumen, which also leads to intestinal obstruction.
- Tumor growth into neighboring organs. Most often, the head of the pancreas is involved in the process. Sometimes it is difficult for clinicians to determine which tumor was primary: intestinal or pancreatic. Only by performing an intraoperative biopsy and immunohistochemical study can the answer to this question be known.
Chemotherapy
If adenocarcinoma cancer cells have spread to the lymph nodes, adjuvant chemotherapy is given after surgery to prevent recurrence. In case of adenocarcinoma with metastases, chemotherapy drugs are used for palliative purposes to slow down the progression of the tumor, improve the patient’s condition, and prolong life.
Combinations of chemotherapy drugs are often prescribed for adenocarcinomas:
- FOLFOX: leucovorin + fluorouracil + oxaliplatin.
- FOLFORI : leucovorin + fluorouracil + irinotecan.
If relapse occurs after surgery, fluorouracil may be prescribed in combination with radiation therapy. This therapy is called chemoradiotherapy .