Esophageal cancer is a malignant tumor that affects the walls of the organ. The tumor body consists of pathologically degenerated epithelial cells. The pathology is characterized by an aggressive course, rapid development, and has an unfavorable prognosis. If we talk about a disease such as esophageal cancer, the first symptoms of the pathology appear quite early, although they are not specific to this particular disease.
The patient feels discomfort after eating, associated with a decrease in the functionality of the affected organ. A cancerous tumor blocks the lumen of the esophagus, as a result of which food cannot move normally. This negatively affects the functioning of all organs of the digestive system, which leads to progression of the clinical picture and deterioration of the patient’s health.
Expert opinion
Sevastyanov Roman
General practitioner, hepatologist, gastroenterologist, highest qualification category. Site Expert
Most often, the pathology is observed in the elderly, with men encountering the problem much more often.
Reasons that can cause the development of an oncological process
The following reasons are identified for the development of esophageal cancer:
- lifestyle features (consumption of hot food, water with a high content of salt and minerals, smoking, alcohol);
- developmental abnormalities - tylosis (a rare genetically determined disease manifested by impaired development of squamous epithelium), sideropenic syndrome.
- precancerous diseases - chronic esophagitis, esophageal ulcers, polyps, Barrett's disease (a disease characterized by the replacement of squamous epithelium with glandular epithelium, characteristic of the stomach).
Causes
The exact causes of esophageal cancer have not been established, but scientists have concluded that external factors, such as frequent consumption of hot food and alcohol, may contribute to the appearance of the tumor. Most often, people living in Iran, China, and Central Asia encounter a malignant or benign tumor of the esophagus, which indicates such factors as eating a large amount of marinades, seasonings, molds and nitrosamines, along with a lack of fresh vegetables and fruits in the diet, as well as selenium.
Risk factors include vitamin deficiencies, especially a lack of vitamins A and C in the body. Smokers are four times more likely to encounter pathological cell degeneration, and in drinkers, esophageal tumors are found twelve times more often. It is not uncommon for an oncological process to develop several years after an alkali burn. In relatively mild diseases such as esophageal achalasia, esophagitis or Barrett's syndrome, there is a ten percent chance of carcinoma occurring.
We recommend reading Intramural uterine leiomyoma - types, indications for surgery, treatment
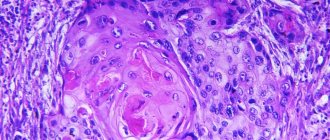
What are the morphological forms of esophageal carcinoma?
The danger of any tumor is determined by how differentiated its constituent cells are.
For esophageal cancer, there are two main forms of pathology:
- The non-keratinizing form is the uncontrolled proliferation of undifferentiated cells. These forms are highly malignant. They grow quickly and metastasize early. Non-invasive forms of squamous cell carcinoma are considered the most malignant tumors.
- Keratinizing cancer is an accumulation of highly differentiated and moderately differentiated cells, therefore the malignancy of this form of cancer is lower.
Stages of the cancer process in the esophagus
There are V degrees of cancer process.
Grade 0 is the emergence of a cancer cell; it is impossible to clinically identify this stage (the words “grade” and “stage” in oncology are now used as synonyms).
Table 1. Characteristics of stages of development of esophageal cancer
| Process characteristics | Stage I | Stage II | Stage III | IV stage |
| Histological characteristics of the stage | The tumor grows deep into the mucous membrane, but does not affect the muscular layer | The mucous and muscular lining of the esophagus is affected. There is a narrowing of the lumen | Swallowing problems, weight loss, and other signs of cancer are prominent. The tumor has grown through all layers of the esophagus | The tumor grows into all membranes of the organ |
| Metastases to regional lymph nodes | No | Single metastases may occur* | Multiple metastases | Multiple metastases |
| Metastases to distant lymph nodes | No | Eat | ||
| Damage to anatomically close organs (trachea, bronchi, vagus nerve, heart) | Does not affect | Does not affect | The tumor grows into nearby organs | |
| Damage to anatomically distant organs (kidneys, liver) | Does not affect | Metastases to distant organs | ||
*For stage 2 esophageal cancer, there are 2 substages:
- II A – no metastases;
- II B – metastases are in the nearest lymph nodes.
Development and dissemination of the process
At the first stage, the disease does not manifest itself with significant symptoms, so the patient is unlikely to suspect health problems. It is possible to identify squamous cell carcinoma of the esophagus (non-keratinizing, keratinizing) only if a person undergoes a preventive examination or came to the clinic with other diseases, during the clarification of which he was referred for a specialized check. Instrumental techniques that help determine the presence of atypical cells: CT, ultrasound, endoscopy.
For squamous cell carcinoma of the esophagus, survival directly depends on the level of progression of the condition. The worst prognosis is for people who sought help at the fourth stage: there are no known cases that resulted in a complete cure. To clarify the level of development, samples of degenerated tissues are taken for histological analysis. In the final stages, the disease spreads to nearby tissues and organs - this is typical of all malignant processes. Possible damage to the trachea, vascular system, bronchi. Metastases are detected not only in the sternum, but also in distant areas of the body.
How do symptoms of esophageal cancer manifest in women?
The earliest symptoms of esophageal cancer are: weakness, loss of appetite. But patients usually do not go to the doctor with these complaints.
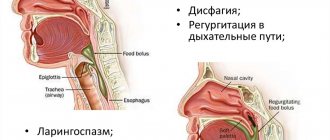
The first symptom of concern is increasing dysphagia (impaired swallowing of food). There are several degrees of dysphagia:
- the patient has difficulty swallowing solid food;
- difficulties arise when swallowing food diluted with liquids;
- difficulty swallowing liquid food;
- the patient cannot swallow anything.
Dysphagia is accompanied by increased salivation.
As the tumor grows and goes beyond the anatomical limits of the organ, the following, already late, signs appear.
Late clinical manifestations include:
- pain first appears when eating, and then becomes constant, the nature of the pain is different, localized in the front, in the upper part of the sternum, or behind, in the interscapular region;
- patients complain of a “lump” behind the sternum;
- when moving to the stomach - constant belching, followed by regurgitation mixed with blood, nausea, vomiting;
- with tumor invasion into the trachea – change in voice timbre;
- when a neoplastic formation grows into the bronchi, aspiration pneumonia often develops, and a sharp hacking cough appears;
- Growth into the mediastinum is characterized by the phenomenon of mediastinitis (inflammation of the mediastinal tissue.
In the terminal stage, the clinic is joined by organs affected by metastasis (liver, bones, lungs).
Prevention of occurrence
If we take into account the causes of the tumor, it is possible to identify preventive measures. This is medical and personal prevention of the disease.
Personal prevention consists of giving up bad habits: using tobacco products, alcoholic beverages, abstaining from spicy foods and spices, maintaining a normal temperature for the food consumed.
The diet includes the required amount of vegetables and fruits that facilitate the movement of food, foods rich in fiber. Don't forget about your oral health. Food that enters the esophagus must be chewed well so that there is no difficulty in swallowing.
Medical prevention consists of periodic examination and treatment of timely detected chronic diseases associated with the gastrointestinal tract, leading to inflammation of the esophageal mucosa.
How does esophageal cancer spread?
Tumor cells are able to move throughout the body, thereby affecting nearby organs, lymph nodes and distant organs.
Ways of spread of cancer cells in the human body:
- Local spread is the growth of a cancer tumor into organs located in anatomical proximity (heart, trachea, recurrent nerve, bronchi).
- Hematogenous spread (through the blood) - cancer cells enter the bloodstream and attach to other organs (the kidneys and liver are most often affected).
- Lymphogenic type of spread is the most important route of metastasis, occurring through the lymphatic vessels. Metastases (secondary tumors) in the lymph nodes closest to the organ are detected already when the tumor has invaded the submucosal layer. In many ways, the localization of metastasis depends on the location of the tumor.
If the tumor is located above the bifurcation (branching) of the trachea, metastasis occurs in the supraclavicular lymph nodes and mediastinal lymph nodes. With distal localization (below the branching) of esophageal cancer, metastasis occurs in the lymphatic collectors of the peritoneum.
But due to the characteristics of the lymphatic system of the esophagus and the presence of retrograde lymphatic flow, metastases at any location of the cancer process can be detected in various lymph nodes.
Causes of squamous cell carcinoma
The causes of squamous cell carcinoma are the same as for other types of malignant tumors. Certain mutations occur in cells that lead to malignant degeneration. “Incorrect” cells lose the external features and functions of normal ones, begin to multiply uncontrollably, and acquire the ability to spread throughout the body.
The main risk factors for squamous cell carcinoma:
- On the skin, such tumors often arise due to the action of ultraviolet rays. Exposed areas of the body are the most vulnerable.
- Squamous cell carcinoma of the genitals, head and neck is caused by certain types of human papillomavirus.
- The risk of developing squamous cell carcinoma is increased in smokers and people who drink a lot of alcohol.
- The likelihood of developing cancer increases with age as mutations accumulate in the cells of the body.
- Scars, burns, chronic inflammation.
- Exposure to certain carcinogenic substances, for example, if a person works in an industrial environment and comes into contact with chemicals.
- Decreased immunity.
None of these factors is guaranteed to lead to the disease - each of them only increases the likelihood to a certain extent.
Diagnosis of esophageal cancer
The diagnosis of esophageal cancer is considered established if cancer cells are found in a biopsy taken from the patient's esophagus. All other examination methods are aimed at clarifying the localization and prevalence of the process. This is necessary for drawing up a patient management plan and choosing a rational method of treatment.
X-ray examination with contrast of the esophagus is performed for all patients with diseases of the esophagus:
- The x-ray clearly shows narrowing of the esophagus; the presence of ulcers and fistulas characteristic of a cancerous process is determined;
- X-rays can be used to determine the position of the cancerous defect relative to other structures and organs;
- the study allows you to assess the patency of the esophagus and its propulsive function (ability for peristaltic movements);
- determine the presence of other diseases of the esophagus.
Esophagoscopy allows not only to take a targeted biopsy of the mucosa for histological examination, but also to examine the affected area in detail, identifying areas of necrosis, ulceration, and bleeding.
CT and MRI are necessary to detect cancer invasion into nearby organs (heart, aorta).
In addition, it is determined whether the cervical lymph nodes and mediastinal lymph nodes are involved in the process, which is extremely important when planning the operation.
Ultrasound computed tomography can detect damage to lymph nodes and anatomically distant organs.
An intraorgan ultrasound examination of the esophagus is done to determine the depth of the oncological process, as well as to assess the condition of the lymph nodes in the peri-esophageal and perigastric space.
Diagnostics
During a visual examination, the doctor does not diagnose the presence of the disease. Before prescribing productive treatment, a diagnosis is carried out using special tools. A tumor of the esophagus can be detected by X-ray with a contrast agent (barium). The solution envelops the organ, and the image shows disturbances in the normal structure.
X-rays help visually determine the degree of narrowing of the esophagus, identify any changes in wall thickness or the presence of ulcerative wounds.
Using an endoscope, the doctor examines whether the wall has spasms or swelling. This examination technique helps to identify the stage of the oncological process, the presence or absence of metastases in the lymph nodes and nearby organs.
Using ultrasound, the exact size of the tumor and secondary formations, if any, are recorded.
To determine the presence of histology, an abdominal biopsy is performed. A laparoscope equipped with a video camera is inserted through a puncture near the navel, and biological material is collected.
To determine an accurate diagnosis, they take a general biochemical test of blood and urine and monitor the dynamics of changes in indicators. Such studies are needed during chemotherapy to monitor the level of red blood cells, platelets, and white blood cells. Diagnosis of tumor-like formations is carried out for comparison with diseases that cause dysphagia.
Principles of treatment and life prognosis
If the oncological process in the esophagus is not treated, then, according to experts, the clinical picture quickly increases and death occurs within 8–9 months from the onset of the first signs of the disease.
Treatment of esophageal cancer is based on three components:
- surgical interventions;
- taking medications;
- radiotherapy.
The treatment tactics for a particular patient are determined by the attending physician, based on the diagnosis, localization and extent of the process. There is no single treatment regimen.
Surgical treatment
The only hope for complete relief from the disease is removal of the tumor along with all affected tissue.
Indications for surgery:
- high degree of differentiation of the cancerous tumor, exophytic tumor growth (into the lumen of the organ);
- localization of the tumor within the organ and lack of invasion into other organs.
The following surgical methods exist:
- Minimally invasive organ-saving surgeries. They are performed through a small laparotomy window in the abdominal wall. The operation is performed using an endoscope. Methods for tumor removal can be different (mucosectomy, electroresection, laser destruction). The operation is only feasible for grades I and II of the disease.
- Radical surgery (Lewis operation). Most often, subtotal resection of the affected part of the esophagus is used, with replacement of the removed part of the esophagus with the missing fragment formed from an intestinal flap. The operation is completed with bilateral (on both sides) 2-3 zone lymph node dissection (removal of fatty tissue with lymph nodes).
If a patient has an inoperable tumor of the esophagus, then to prolong life and to establish enteral nutrition, palliative operations are performed:
- gastrostomy - placement through the abdominal wall of a gastric fistula to feed the patient without going through the esophagus;
- bypass anastomosis - the creation of an artificial esophagus from a segment of intestine that goes around the affected area;
- esophageal stenting – insertion of a rigid tube into a section of the esophagus reduced in diameter.
The prognosis after surgery is individual and depends on many conditions. Therefore, we can only talk about statistical survival rates:
- with stage I cancer, almost all patients survive 5 years;
- with stage II cancer, slightly more than half of patients survive 5 years;
- with stage III cancer, only every tenth patient who underwent esophageal resection for cancer survives the five-year mark.
- For stage IV cancer, surgical treatment is not effective and death occurs quickly.
Treatment
Treatment consists of selecting strengthening therapeutic procedures, the necessary diet, and prescribing one or more generally accepted cancer treatment methods.
Carrying out a surgical operation
Until recently, surgery was considered the only effective method by which it was possible to stop the development of oncology and defeat the disease. Currently, to perform an operation, it is necessary to have appropriate indications and the absence of contraindications. Main types of operations: esophageal stenting, Lewis-Ivor operation.
When performing stenting, the surgeon places a special stent in the patient’s esophagus, which stops food trauma to the tumor and preserves the lumen of the esophagus, but there is a risk of damaging the mucous layer. The doctor assesses the need for surgery based on the likelihood of consequences. After surgery, it is important to follow all medical recommendations for a speedy recovery.
Radiotherapy
Use of high doses of radioactive radiation for the treatment of oncology. There is a contact and non-contact method of exposing cancer to radiation. A lot of health consequences have been established when using this method, since radiation causes changes in healthy cells along with atypical ones. It is rarely used as an independent method of treatment.
Chemotherapy
Pharmacological drugs with cytostatic action are used. As a result of a course of use, the atypical cell is stopped and destroyed. 3-6 courses of drug administration are prescribed with an interval of 2-4 weeks. By nature, cytostatics are a toxic substance, which causes severe side effects and negatively affects the patient’s health. The use of strengthening therapy is necessary. The body is poisoned, but at the same time the rate of development of pathology and the size of the tumor slows down.
Chemotherapy for esophageal cancer
Chemotherapy carried out for oncological processes has different goals:
- As the main method of treatment when surgery is not indicated. In this case, the goal is to reduce the intensity of tumor growth, which ultimately affects the improvement of the patient’s condition and prolongation of his life.
- Neoadjuvant therapy is prescribed before surgery in order to reduce its size and more clearly see the boundaries of the tumor during surgery.
- Adjuvant chemotherapy is prescribed after surgery. It completes the success of surgical treatment by preventing relapse of the disease.
- Chemoradiation therapy is chemotherapy and radiation therapy combined. The combination of two methods in some cases significantly increases the effectiveness of treatment.
General chemotherapy is most often used, when the drug is injected into a vein or taken orally in the form of tablets.
Radiotherapy for malignant tumors of the esophagus
Radiotherapy is widely used in the treatment of esophageal cancer. Ionizing radiation is considered the most effective. Ionizing rays can act on mutated cells without affecting healthy tissue. The effect of radiation can be represented schematically:
- damaging effect on carcinoma cells;
- the development of irreversible processes in tissues that have undergone cancer transformation under the influence of radiation therapy;
- replacement of destroyed tumor cells with healthy tissue.
This is not a one-time process, so the results of radiation therapy are judged after some time.
In radiotherapy, depending on its goals, there are the following areas:
- radical radiation therapy – it is aimed at maximizing the patient’s cure from the oncological process, using large doses of radiation;
- palliative radiation therapy, used for inoperable forms of esophageal cancer, to prolong the patient’s life;
- symptomatic radiotherapy – reduces the severity of the main symptoms of the disease.
During treatment, the source of ionizing radiation can be outside the patient’s body (remote method), or can be introduced into the cavity of the esophagus, which increases the therapeutic effect and makes it possible to increase the radiation dose without damaging healthy tissue.
The combined method is used to increase the effectiveness of treatment; remote treatment and brachytherapy (contact method) are performed simultaneously.
The long-term results of radiation therapy are very far from satisfactory. According to statistics, when only radiation therapy is used, life expectancy is low, the percentage of five-year survival ranges from 3 to 8%.
Dietary regimen for esophageal cancer
Malnutrition and, as a consequence, low weight are common to all patients with esophageal cancer. As the process progresses, eating becomes a difficult task. Malnutrition negatively affects the physical and mental health of the patient.
The menu for esophageal cancer should be rich in proteins (meat, poultry, fish, milk, eggs) and energy products (oatmeal, bread and pasta made from unrefined flour, brown rice). The patient’s daily menu should contain vitamin products, crushed in a blender (berries, herbs, fruits), as well as animal and vegetable fats (butter, cream, vegetable oil). The patient should eat small portions, but often. The food should be warm.
Methods of eating during this disease depend on the severity of the disease, as well as on the treatment carried out at this time.
Treatment for second stage cancer is complex and includes all three components. Before starting treatment, it is necessary to regain weight and maintain it during treatment. The diet for stage 2 cancer is the natural and enteral route:
- With natural nutrition, pureed, semi-liquid food enters through the mouth. Multiple meals, in small portions.
- Enteral. As the tumor grows, nutrition through the mouth becomes unavailable. Then nutrition is provided through a tube, which is inserted through the nose into the jejunum or stomach. After surgery, a tube is placed in the jejunum (jejunostomy) to deliver food to the body as soon as possible after surgery.
For stage 3 disease, treatment mainly includes radiation and chemotherapy. Radical operations are rarely performed for stage 3 cancer. In order to enable the patient to eat, a stenting operation is performed. Nutrition through the stent should be complete, with plenty of protein.
In the fourth stage, when chemotherapy remains in the treatment arsenal, the patient is also fed through a stent.
Esophageal cancer is a serious, deadly disease. But with early detection, the likelihood of overcoming the disease is quite high. Therefore, the main recommendation of oncologists is to immediately consult a doctor at the first signs of the disease.
Symptoms
There is no clinical picture of an esophageal tumor at the initial stage; sometimes it may seem to a person that food is sticking to the walls of the esophagus. A slight sore throat may also be present. When a benign tumor in the esophagus grows, dysphagia (difficulty swallowing food) develops. In case of malignant formations, cancer intoxication, which occurs as a result of tumor disintegration, is added to the symptoms. The main symptoms of neoplasms are:
- swallowing function is impaired;
- tickle in the throat;
- it becomes difficult to take even liquid food;
- there is a feeling as if there is a foreign body in the organ;
- nausea and vomiting occurs, sometimes with blood;
- salivation increases;
- pain occurs behind the sternum, becoming more intense during meals;
- weakness, dizziness, and fatigue occur;
- weight suddenly decreases;
- iron deficiency anemia develops.
We recommend reading: How to treat hygroma on the leg
In the absence of timely treatment, the esophageal canal becomes completely blocked, even liquid food becomes impossible to swallow, due to the disintegration of the tumor, internal bleeding occurs, the walls of the organ become thinner and covered with ulcers. The patient notes the occurrence of paroxysmal cough, fistulas appear in the affected part of the esophagus, which gradually spread to the mediastinum. With metastasis to the neck, brain, lungs, bones, liver and other organs, corresponding symptoms occur.