Causes of bile stagnation
Why does bile stagnation occur? Some people, having heard the term “cholestasis,” have no idea what it is or why this disease develops. The causes of the disease we are considering are extremely diverse. In general, cholestasis syndrome can occur in a variety of conditions:
- alcoholic liver damage;
- viral liver damage;
- toxic liver damage;
- drug-induced liver damage;
- benign form of recurrent cholestasis;
- disturbances in intestinal microecology;
- cirrhosis of the liver;
- cholestasis of pregnancy;
- bacterial infections;
- endotoxemia;
- biliary primary cirrhosis;
- Caroli's disease;
- sclerosing primary cholangitis;
- biliary atresia;
- tuberculosis;
- sarcoidosis;
- lymphogranulomatosis;
- Idiopathic ductopenia.
Canalicular and hepatocellular cholestasis lead mainly to lesions of transport membrane systems; extralobular cholestasis occurs when the epithelium of the bile ducts is damaged.
Treatment
The most effective treatment for both intrahepatic and extrahepatic cholestasis is considered etiotropic therapy , primarily aimed at eliminating the causes. Ursodeoxycholic acid also gives good results, including in cases of liver cirrhosis caused by alcohol poisoning.
To eliminate skin itching, plasmapheresis and opioid antagonists are used in the treatment of the disease.
Since cholestasis is accompanied by hypovitaminosis, which entails side effects that require separate treatment, it is necessary to take vitamins K, D, E and fat-dissolving drugs.
If the obstruction in the bile duct is mechanical in nature or the bile ducts are blocked , then, in addition to conservative treatment, surgical intervention (conventional or endoscopic) is required.
Complications and consequences of cholestasis
With cholestasis, the process of copper metabolism in the body is disrupted. In a healthy state , the body excretes 80% of copper in feces , but during cholestasis, copper remains in the body, causing pigmentation of the cornea. Another consequence of cholestasis is disruption of the cardiovascular system, which leads to arterial hypotension, problems with blood clotting, increased bleeding and an increased risk of sepsis.
In addition, cholestasis provokes diseases such as:
- osteoporosis;
- hemeralopia (decreased vision at dusk, or night blindness);
- the occurrence of stones in the gall bladder and/or bile ducts;
- development of inflammation of the bile ducts (cholangitis);
- liver failure;
- cirrhosis.
Classification
The etiology and pathogenesis of cholestasis in adults is determined by many factors. Depending on the reasons, there are two main forms:
- extrahepatic cholestasis is formed due to mechanical obstruction of the ducts; the most common etiological factor is bile duct stones;
- intrahepatic cholestasis develops in diseases of the hepatocellular system, as a result of damage to the intrahepatic ducts, or combines both links. With this form there is no obstruction or mechanical damage to the biliary tract.
The intrahepatic form is further divided into the following subtypes:
- hepatocellular cholestasis, which causes damage to hepatocytes; canalicular, occurring with damage to membrane transport systems;
- extralobular, associated with a violation of the structure of the ductal epithelium;
- mixed cholestasis.
The manifestations of hepatic cholestasis syndrome are based on one or more mechanisms: the entry of bile components into the bloodstream in excess, a decrease or absence of it in the intestine, the action of bile elements on the tubules and liver cells.
As a result, bile enters the blood, causing symptoms and damage to other organs and systems.
Depending on the nature of the course, cholestasis is divided into acute and chronic. Additionally, there are several types:
- partial cholestasis – accompanied by a decrease in bile secretion;
- dissociated cholestasis – characterized by retention of individual components of bile;
- total cholestasis - occurs with a violation of the flow of bile into the duodenum.
Also, this syndrome can occur in anicteric and icteric forms.
Cholestasis during pregnancy
What causes intrahepatic cholestasis in pregnant women is not clear. There are a number of theories that identify the main groups of reasons:
- increased sensitivity to sex hormones of liver cells due to genetic disposition;
- the normal synthesis of enzymes that ensure the transport of bile from cells through the ducts is disrupted;
- the synthesis of bile acids is impaired from birth due to a deficiency of certain enzymes. This disorder can cause the formation of atypical bile acids.
The main changes in pregnant women with the syndrome:
- the amount of bile components in the blood is increased;
- the level of secretion in the duodenum is reduced;
- on the part of bile, there is an effect on hepatocytes and biliary tubules.
Symptoms of the disease in pregnant women, which begin to appear by the third trimester, are irritation and jaundice. In some patients, skin itching can be pronounced and cause a lot of inconvenience, while others tolerate it easily. Intrahepatic cholestasis leads to excoriation of the skin in pregnant women, usually on the arms, legs, and forearms. Symptoms of jaundice appear in only a tenth of women; usually these signs disappear on their own after two weeks after the baby is born. Still, you should not rely on the fact that everything will go away on its own; if you feel any changes in your health, you should consult a doctor, since all the signs can reappear due to hormonal imbalance.
Treatment of pregnant women is complicated by their piquant situation, so non-traditional treatment methods, such as oatmeal masks and chamomile decoction, are used to reduce symptoms. You can even use cold water; it relieves the condition by slowing down the blood flow, so the urge to itch decreases. It is recommended to sleep in a cool room, as well as follow a diet.
Pediatric cholestasis
The causes of childhood cholestasis may be metabolic disorders from birth, consequences of viral diseases, cardiovascular failure, malignant pancreatic tumors, parasitic lesions, genetic predisposition, sclerosing cholangitis.
The manifestation of cholestatic syndrome in children depends on the age at which the disease began and the characteristics of the body. The disease should be treated after the root cause of the disease has been eliminated. For example, if bile stagnation is caused by a malignant neoplasm, then you need to fight the tumor first, and then the symptoms of the syndrome. The child’s therapy is comprehensive: in addition to medications, vitamins A, E, D, K, as well as choleretic drugs can be prescribed.
Often, cholestasis in this group of patients cannot be cured with medications alone; then a surgical operation is performed, which is aimed at removing stones and draining blocked ducts. The danger of cholestasis is that it develops in children in a latent form. To avoid complications and severe forms of the condition, you need to start treatment in a timely manner.
Symptoms of bile stagnation
Cholestasis, due to the excessive concentration of bile components in the liver, as well as in the tissues of the body, provokes the occurrence of hepatic and systemic pathological processes, which, in turn, determine the corresponding laboratory and clinical manifestations of this disease.
Symptoms of bile stagnation in the body, characteristic of cholestasis, are determined by the underlying disease, as well as hepatic cell failure and impaired excretory functions of hepatocytes. The following signs of the disease are identified:
- itching of the skin is the main (and for a long time the only) symptom of the disease. As a rule, itching bothers you at night and decreases during the day. Some patients report increased itching in winter;
- xanthomas (small yellow or brownish formations, most often located on the chest, back and elbows). The appearance of xanthomas is associated with the deposition of lipids (fats), which are markers of cholestasis;
- xanthelasmas (small yellow or brownish formations located symmetrically on the eyelids). Their appearance is associated with disorders of fat metabolism in the body;
- scratching of the skin (arising from severe itching), pustular rashes;
- jaundice (yellow discoloration of the skin, mucous membranes (eyes, mouth), sclera of the eyes);
- hyperpigmentation of the skin (increased color, darkening) due to the deposition of melanin (a special chemical compound that gives the skin color);
- steatorrhea (excretion of large amounts of fat in stool). Its appearance is due to insufficient absorption of fats in the intestines, as a result of which the feces become liquid, greasy, mushy, with an unpleasant odor, and are difficult to flush from the walls of the toilet;
- changes in the color of stool and urine (darkening of urine and discoloration of stool);
- increased bleeding, which is associated with decreased absorption of fat-soluble vitamin K in the intestine;
- Hypovitaminosis is a deficiency (lack) of vitamins in the body. Hypovitaminosis in cholestasis is associated with impaired absorption of fat-soluble vitamins in the intestine (A, D, E);
- weight loss;
- cholelithiasis (formation of stones in the gall bladder and bile ducts).
The long course of cholestasis is often complicated by the formation of pigmented stones in the biliary system, which, in turn, are complicated by bacterial cholangitis.
The formation of biliary cirrhosis determines the relevance of signs of hepatic cellular failure and portal hypertension. Anorexia, fever, vomiting and abdominal pain may be symptoms of the disease that causes cholestasis, but they are not symptoms of the disease itself.
Treatment methods
Treatment of cholestasis is based on therapeutic methods aimed at the underlying disease, normalizing the movement and synthesis of bile, eliminating the symptoms of the disease. For cholestasis caused by intoxications, drugs and alcohol, it is necessary to eliminate the impact of a negative factor on the body - avoid alcohol, drugs, contact with chemicals .
Since the first symptom is most often unbearable itching, it must be eliminated. Various drugs are used for this:
- Phenobarbital.
- Cholestipol.
- Rifampicin.
- Ursofalk.
- Heptral.
For treatment, hepatoprotectors with a choleretic effect must be selected: Ursofalk, Hofitol, Allohol, Heptor, Liv 52. The hepatoprotector Ursofalk not only effectively relieves itching, but also has other therapeutic effects due to its composition.
Ursodeoxycholic acid, the active substance of the drug, is part of the bile acids formed in the human body, so its intake has a protective, immunostimulating and choleretic effect on liver cells.
Also, taking the drug ensures the softening of cholesterol formations in the ducts and gall bladder. An analogue of Ursofalk in terms of the active substance is the drug Ursosan, which has a similar composition and therapeutic effect.
In case of damage to the ducts, disruption of the secretory function of hepatocytes and the threat of development of the fermentation process in the intestines, the drug Allohol is prescribed, which improves digestion, stimulates lipid metabolism, increases the volume of bile secreted and normalizes intestinal function.
For hepatocellular and canalicular cholestasis, drugs with ademetionine are prescribed - Heptral, Heptor, Methionine. Such drugs normalize blood biochemistry, have a mild antidepressant effect, and have a biliary and regenerative effect. Most often prescribed to patients with alcohol and nicotine addiction, suffering from viral hepatitis.
Other drugs:
- Glucocorticosteroids – Metypred, Prednisolone, Medrol.
- To lower cholesterol - Zocor, Atoris, Crestor.
- Vitamins K, D, C, E, A, group B.
- Calcium gluconate tablets or injections.
- Cytostatics – Methotrexate.
- Antiviral: Viferon, Interferon, Ribavirin.
In many cases, especially if cholestasis is diagnosed in the early stages, it can be completely cured. But when the process is running, it is aimed at stopping the progression of the pathological process and relieving symptoms. In many ways, the success of treatment depends on the patient himself - whether he is ready to give up bad habits and adhere to a therapeutic diet.
Doctor's review: “Clinical studies and the experience of practicing specialists show that the use of drugs based on ursodeoxycholic acid leads to an improvement in blood counts and a slowdown in the development of the disease. The drug has shown particular effectiveness in the treatment of biliary cirrhosis.”
Diagnostic methods
In order to correctly diagnose cholestasis, it is necessary to undergo a comprehensive examination in a medical institution. It should include the following diagnostic methods:
- analysis of medical history and complaints;
- life history data;
- physical examination. The possible yellowness of the skin and sclera of the eyes and its intensity are determined. The liver is palpated and percussed and its pain is checked. The condition of the skin is assessed;
- blood analysis;
- urine test (bile pigments are detected);
- biochemical blood test (detect hyperbilirubinemia - increased bilirubin in the blood, increased levels of lipids, bile acids, changes in the lipid spectrum, increased levels of alkaline phosphatase);
- ultrasound examination (ultrasound) of the abdominal organs to detect an enlarged liver, changes in the gallbladder;
- computed tomography (CT) and magnetic resonance imaging (MRI) of the abdominal organs, identify possible changes in the liver and gallbladder;
- retrograde cholangiopancreatography (a method for examining the bile ducts to assess their condition);
- percutaneous transhepatic cholangiography (endoscopic examination of the bile ducts after filling them with a radiopaque substance);
- magnetic resonance cholangiography (a method for examining the bile ducts) is the most promising research method due to its high information content;
- liver biopsy (examination of a section of the organ) to identify the cause of cholestasis and possible changes in the liver;
- Consultations with a therapist or hepatologist are also possible.
During a full-fledged study, the doctor decides what to do and what treatment method should be prescribed to the patient.
Cholestasis syndrome
In the peripheral blood, target-like red blood cells, anemia, and neutrophilic leukocytosis are detected. Within 3 weeks, the content of conjugated bilirubin in the blood serum increases. Biochemical markers of cholestasis are alkaline phosphatase and uglutamyl transpeptidase, leucine aminopeptidase and 5-nucleotidase. In chronic cholestasis, the level of cholesterol lipids, phospholipids, triglycerides, and lipoproteins increases, mainly due to the low-density lipoprotein fraction. At the same time, the concentration of high-density lipoproteins is reduced. The serum contents of chenodeoxycholic, lithocholic and deoxycholic bile acids are increased. The level of albumin and globulin does not change in acute cholestasis. The activity of AST and ALT increases slightly. Bile pigments and urobilin are found in the urine.
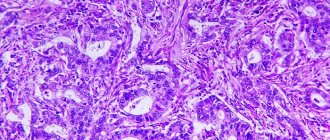
Morphologically, the liver with cholestasis is enlarged in size, greenish in color, with a rounded edge. In later stages, nodes are visible on its surface. Light microscopy reveals 6-irubinostasis in hepatocytes, sinusoid cells, and tubules of the third zone of the lobule. “Cirrus” degeneration of the hepatocyte, foam cells surrounded by mononuclear cells, are revealed. Necrosis of hepatocytes, regeneration and nodular hyperplasia in the initial stages of cholestasis are minimally expressed. In the portal tracts (first zone), proliferation of ductules and the presence of bile thrombi are observed; hepatocytes turn into bile duct cells and form the asal membrane. Obstruction of the bile ducts is promoted by the development of fibrosis. Mallory bodies may form in cholestasis. The microvasculature of the liver and its cellular elements undergo reactive changes. Swelling of the cells lining the sinusoids, their dystrophic changes, and the presence of vacuoles containing bile components or their metabolites are observed. By electron microscopy, changes in bile canaliculi are nonspecific and include dilatation, edema, thickening and tortuosity, loss of microvilli, vacuolization of the Golgi apparatus, and hypertrophy of the endoplasmic reticulum. In the liver (hepatocytes, Kupffer cells, bile duct epithelium) there is excessive deposition of copper and metalloproteins, lipofuscin, cholesterol, and other lipids. Changes in liver biopsy in the early stages of cholestasis may be absent.
In the early stages of cholestasis, the liver is not microscopically changed, in the later stages it increases in size and has a greenish color. Microscopic signs of cholestasis in the liver are clumps of bilirubin in the cytoplasm of hepatocytes and lumps of bile (bile thrombi) in the lumens of dilated bile canaliculi. Rupture of the bile canaliculi leads to the release of bile into the intercellular space with the formation of “bile lakes”. Morphological signs of cholestasis are usually more pronounced in the central zones of the hepatic lobule. With long-term disorders of biliary excretion, these changes are visible in the intermediary and then periportal zones. As already noted, there are three forms of cholestasis: intracellular, intratubular and mixed. In the early stages, one or another form of cholestasis is rarely expressed. Intracellular cholestasis is observed with drug (aminosine ) damage, intratubular - with subhepatic jaundice, mixed - with viral liver damage. Coagulation of bile in the interlobular bile ducts is detected only in sectional preparations.
Hydropic and acidophilic dystrophy in the liver is observed already on the 7th day. In rare cases, the cytoplasm of hepatocytes, located around thrombosed bile canaliculi that do not accept dyes well, appears reticulated and contains pigment granules - “pinnate” degeneration of hepatocytes. Progressive dystrophy leads to necrotic changes in the parenchyma.
The following types of necrosis in cholestasis are distinguished:
- focal necrosis of hepatocytes (sensitivity to staining is reduced, the nucleus disappears, hepatocytes are replaced by leukocytes);
- necrobiosis of a group of hepatocytes in a state of “pinnate” degeneration ends in biliary or reticular (mesh) necrosis;
- centrilobular zonal necrosis of hepatocytes (usually in sectional preparations).
Alteration of the parenchyma is caused by the toxic effects of bile components, as well as mechanical pressure from dilated thrombosed bile canaliculi. Stagnation of bile and necrobiosis of hepatocytes are accompanied by inflammatory mesenchymal cell reactions (they occur no earlier than the 10th day of stagnation), then hyperplasia of reticulin fibers in the lobule and proliferation of connective tissue in the portal field occur - the beginning of the formation of biliary cirrhosis. Stagnation of bile is also accompanied by proliferation of cicholangioles. In the liver tissue, the content of glycogen and RNA is reduced, the amount of lipids is increased, there is a positive PAS action of glycoproteins, protein and its active groups, the activity of oxidoreductases is reduced and CP and ALP are increased. The lumen of the tubules is widened from 1 to 8 μm; there are no villi at the biliary pole of the hepatocyte, or they are shortened and take the form of a balloon or bubble. The ectoplasm of the pretubular zone of the hepatocyte is expanded, the Golgi apparatus is increased in size, and hyperplasia of the smooth ER is noted. The number of lysosomes is increased, they are randomly located in hepatocytes (not only in the peribiliary zone, but also at the vascular pole), and also extend into the space of Disse. Mitochondria show signs of dystrophic changes. The junction of cells in the area of the bile canaliculi appears intact. The ultrastructure of the altered liver is identical to intrahepatic and extrahepatic cholestasis. The existing differences are quantitative: with extrahepatic cholestasis they are more pronounced.
Bile thrombi consist of granular components (bile itself) and ring-plate formations of free bilirubin and have a coarse-grained structure localized in mesosomes. Bound bilirubin, having the form of small grains, is located in the vesicles of the EPS, and sometimes lies freely in the cytoplasm.
There are differences in the nature of damage to the intrahepatic bile ducts in various diseases. VH is characterized by the formation of catarrhal and obstructive cholangitis, PBC is characterized by destructive cholangitis, and subhepatic jaundice is characterized by pericholangitis.
Stagnation of bile in the liver is naturally accompanied by proliferation of cholangioles (ductular proliferation). Proliferating bile ducts may be no different from ordinary bile ducts. Sometimes proliferating bile ducts do not have a clear lumen and are formed by two rows of oval cells with an elongated nucleus and basophilic cytoplasm. A significant number of ducts in the portal field indicates their proliferation.
Proliferation of the bile ducts has an adaptive-compensatory significance and is aimed at correcting bile secretion. When the cause of bile stagnation is eliminated, the ductular reaction is reduced, and the portal triad is completely restored.
The results of clinical and biochemical studies do not always make it possible to distinguish between intrahepatic and extrahepatic cholestasis. The diagnostic examination algorithm is of great importance. Extrahepatic mechanical obstruction with the development of biliary hypertension is supported by pain in the abdominal cavity (observed when stones are localized in ducts, tumors), palpable gallbladder. Fever and chills may be symptoms of cholangitis. The density and tuberosity of the liver upon palpation reflect advanced changes or tumor damage to the liver. The diagnostic examination algorithm involves, first of all, performing an ultrasound of the abdominal organs, which makes it possible to identify a characteristic sign of a mechanical blockade of the bile ducts - suprastenotic dilatation of the bile ducts (the diameter of the common bile duct is more than 6 mm). When dilatation of the ducts is detected, it is advisable to conduct cholangiography. The procedure of choice is endoscopic retrograde cholangiography (ERCH). If retrograde filling of the bile ducts is impossible, percutaneous transhepatic cholangiography (PTCHG) is used. If there are no signs of extrahepatic obstruction of the bile ducts, a liver biopsy is performed. This procedure can be performed only after excluding obstructive extrahepatic cholestasis (to avoid the development of biliary peritonitis). Cholescintigraphy with technetium-labeled iminodiacetic acid also helps to identify the level of damage (intrahepatic or extrahepatic). The use of magnetic resonance cholangiography is promising.
Treatment of cholestasis
How to get rid of an unpleasant illness? Treatment of cholestasis is carried out comprehensively, taking into account the medical history. Etiotropic treatment is indicated when the causative factor is established. Depending on the level of development of intrahepatic cholestasis, pathogenetic therapy is indicated:
- When the permeability of the basolateral and/or canalicular membrane decreases, as well as when Na+, K+, ATPase, and other membrane transporters are inhibited, the use of heptral is indicated. It is based on an active substance that is part of the tissues and fluids of the body and is involved in transmethylation reactions. Heptral has antidepressant and hepatoprotective activity. Antioxidants and metadoxyl are indicated for the same purpose;
- Destruction of the cytoskeleton of hepatocytes and disruption of vesicular transport require the use of heptral, antioxidants, and rifampicin. They are based on the induction of microsomal liver enzymes;
- Changes in the composition of bile acids and disruption of the formation of bile micelles require the use of ursodeoxycholic acid, which helps to reduce hydrophobic bile acids, thereby preventing a toxic effect on hepatocyte membranes;
- For the treatment of skin itching that occurs against the background of cholestasis, CNS opiate receptor blockers and serotonin receptor blockers are effective. For symptoms of osteoporosis, it is advisable to take vitamin D3 in combination with calcium supplements. For severe bone pain, calcium gluconate is prescribed. All patients with the appropriate diagnosis are prescribed vitamin A and vitamin E. For hemorrhagic manifestations, vitamin K is prescribed;
- In some cases, patients are shown methods of extracorporeal hemocorrection: plasmapheresis, leukocytapheresis, cryoplasmasorption, and ultraviolet irradiation of blood. You cannot avoid following a diet - it is important to limit the amount of neutral fats to 40 grams per day, fill the diet with vegetable fats, margarines containing medium-chain triglycerides.
Treatment process
All patients with cholestasis syndrome are advised to follow a strict diet. Animal fats must be excluded from the diet. It is permissible to consume foods containing vegetable fats. Their absorption does not require the presence of bile acids. Prohibited are smoked meats, fatty meats, sausages, baked goods, sweets, ice cream, canned food, marinades, pickles, mushrooms, sauces, spices, spicy foods, beans, citrus fruits, nuts, sour fruits and berries, chocolate, canned food, cooking fats, fast food -food, semi-finished products, carbonated and alcoholic drinks. Food must be taken in small portions - 5-6 times a day in small portions every 3-4 hours. You should prepare dishes that are easy to digest and contain many vitamins and minerals. Food must be eaten warm. The diet should be enriched with foods that prevent constipation and contain a lot of magnesium to stimulate bile flow. Cooking food by steaming, baking, stewing or boiling is shown.
Drug treatment consists of prescribing the following groups of drugs:
- Hepatoprotective agents - “Essentiale Forte”, “Karsila”, “Phosphoglyph”;
- Cytostatic drugs - Methotrexate, Cyclophosphamide, Tamoxifen;
- Cholelitholytics – “Ursofalka”, “Ursosana”;
- Choleretic agents – “Hofitola”, “Allochola”;
- Enzymes – “Creona”, “Mezima”;
- Antihistamines – “Suprastina”, “Zodaka”, “Zirteca”;
- Corticosteroids – “Prednisolone”, “Hydrocortisone”;
- Antioxidants – “Actovegin”, “Riboxin”, “Trimetazidine”;
- Fat-soluble vitamins and calcium.
To treat skin itching, blood purification is used by plasmapheresis, hemosorption, ultraviolet irradiation, and cryoplasmasorption.
drainage of bile ducts
Surgical intervention is carried out to eliminate the causative factors that caused bile stagnation . To restore the normal flow of bile, surgeons perform anastomoses, install drainages in the bile ducts, remove stones, excise tumors, install stents and cut adhesions. Endoscopic or traditional surgical treatment is indicated for all patients who have an obstruction in the biliary tract that prevents the normal flow of bile. In extreme cases, when liver function is significantly impaired, an organ transplant from a donor is performed.
Rehabilitation measures:
- Electrophoresis,
- Diadynamic therapy,
- exercise therapy,
- Massage,
- Spa treatment.
The prognosis for recovery from cholestasis is favorable. Early diagnostic procedures and a competent approach to treating patients make it possible to achieve complete recovery and achieve stable remission. To prevent the development of pathology, it is necessary to adhere to the principles of proper nutrition and promptly treat diseases of the hepatobiliary system.
Cholestasis is a signal that the body has a serious illness that requires special attention from doctors and the provision of qualified medical care in the form of prescribing an adequate treatment regimen.
Cholestasis in children
As a rule, in children most often we are talking about the development of intrahepatic cholestasis, less often - extrahepatic. In the vast majority of cases, the causes of the development of extrahepatic cholestasis are congenital malformations of the bile ducts: atresia or stenosis of the common bile duct.
Cases where there is an internal obstruction to the outflow of bile (closing the lumen with gallstones) are quite rare in pediatric practice.
One of the very first external signs that can be identified immediately is severe and constant skin itching, accompanied by a rash, however, this symptom is most often observed in adolescents; it is much less common in young children.
A common sign of cholestasis in very young children is jaundice, and it can be determined by the uniform yellowish tint of the skin of the entire body, as well as the face. In addition, the mucous membranes and whites of the eyes acquire a yellowish tint.
Cholestasis syndrome in a child is stagnation of bile in the ducts of the gallbladder, which leads to the development of severe intoxication of the body, the formation of stones, allergic reactions, and liver poisoning.
Diagnosis and treatment of this type of disease is carried out in a hospital setting. The doctor of the department of gastroenterology and pulmonology, based on the results of biochemical and general blood tests, as well as ultrasound diagnostic data, decides how to treat this pathology.
The therapeutic approach may include:
- diet prescription;
- choleretic and liver treatment drugs;
- antibiotics for fever;
- antihistamines; drugs to stabilize digestive function;
- probiotics, prebiotics;
- vitamin complex and folic acid; sorbents;
- in rare cases, surgery is performed to correct the malformation.
The specialist’s main recommendation is to avoid fatty and unhealthy foods and follow a diet.
Cholestasis in pregnancy
Separately, it is worth mentioning such a pathology as intrahepatic cholestasis, which arose as a result of hormonal imbalance during pregnancy. This disease in pregnant women is relatively rare , however, it can harm the body of both the mother and the fetus. The prognosis for a pregnant woman is usually favorable - cholestasis develops mainly in the third trimester and disappears almost immediately after childbirth. However, the risk of intrauterine fetal death increases to 15%.
The causes of the disease are still unclear. Experts identify three potential groups:
- excess estrogen , which during this period, in particular towards the end of pregnancy, in a woman’s body increases 1000 times;
- compression of the gallbladder and liver by the pregnant uterus (it is in the last trimester that it reaches its maximum size);
- the hereditary nature of the disease (more than half of the women in the family had such pathologies).
In addition, there are factors that also influence the development of cholestasis in pregnancy. If a woman has already suffered cholestasis of pregnancy, then the risk of recurrence during subsequent pregnancies increases to 70%. Liver diseases before pregnancy increase the possibility of cholestasis during pregnancy. In addition, the occurrence of cholestasis is higher in multiple pregnancies and pregnancies resulting from in vitro fertilization, as well as in the presence of close relatives who have suffered from this disease.
Symptoms of cholestasis in pregnancy
- severe itching, especially on the palms and soles of the feet;
- dark urine and light feces;
- jaundice.
Symptoms can appear all at once or one at a time, but most often the only symptom is itching.
Complications of cholestasis in pregnancy
The main complications of the disease in the mother are problems with the absorption of fat-soluble vitamins (A, D, E and K) , unbearable itching and an increased risk of relapse during subsequent pregnancies.
For a pregnant child, there are many more complications. First of all, there is a risk of premature birth for reasons that are still unclear. Further, there is a chance that the baby will inhale meconium during birth, which will cause breathing problems . The risk of intrauterine fetal death is also increased. Therefore, doctors often induce premature birth to avoid complications for the baby.
Diagnosis and treatment of cholestasis in pregnancy
When making a diagnosis, doctors rely on the results of interviewing the pregnant woman about the presence of symptoms of the disease and personal and family medical history, a physical examination, blood tests, measuring the level of bile in the blood, and ultrasound.
Treatment consists of relieving symptoms, primarily itching, and preventing possible complications. In this case, ursodeoxycholic acid preparations, as well as corticosteroids in the form of creams or lotions that relieve itching, are successfully used.
Signs on ultrasound
The simplest and most informative method that allows you to determine cholestasis and its causes is ultrasound examination. An ultrasound can show the presence of a stone, its location and size, and visualize the expansion or narrowing of the bile ducts. The technique is used to identify cysts and tumor formations in all internal organs of the abdominal cavity. In case of diseases of the gallbladder, its size, wall thickness, and the condition of the internal surface are assessed.
Signs of cholestasis on ultrasound are not considered specific, but when they are identified, cholangiography is used as a more reliable method. If cirrhosis or cancer is suspected, a liver biopsy is performed.
Itching as the main symptom
When cholestasis appears, its symptoms, regardless of origin, are general. The patient notes:
- weakness and signs of intoxication due to increased bilirubin;
- lightening of stool and darkening of urine;
- muscle and joint pain;
- the formation of subcutaneous xanthomas and xanthelasmas, which are accumulations of cholesterol;
- yellow discoloration of the skin and mucous membranes;
- nausea, heartburn, vomiting, abdominal pain and constipation.
All signs of cholestasis syndrome are not specific and may accompany other diseases.
The main symptom of impaired bile outflow is skin itching with cholestasis of varying intensity. At times it can be so unbearable that a person’s sleep and appetite are disrupted and the quality of life sharply decreases. This sensation intensifies at night and after swimming. The mechanism of this phenomenon has not yet been sufficiently studied; there are several theories for the appearance of itching:
- Accumulation of toxic bile acids under the skin. However, there is no clear relationship between their level in the blood and the severity of this symptom.
- An increase in the amount of endogenous opioids in a patient with liver damage. When antagonists of these substances are prescribed, many patients experience a decrease in itching.
- Increased lysophosphatidic acid in blood serum. Animal studies have confirmed the relationship between itching and the level of this substance.
Treatment with folk remedies
Almost every thematic forum contains a variety of advice on the alternative treatment of cholestatic syndrome. However, before using such advice, it is important to consult your doctor. After all, choleretic herbs in the presence of stones can significantly worsen the condition.
- Collection of herbs . Corn silk, rose hips, dandelion, barberry, mint, dill, wormwood, tansy, calamus, plantain, chicory, and yarrow have choleretic properties. A collection of several herbs or decoctions of each of them should be prepared at the rate of 1 tbsp. l. dry product per 1 tbsp. water. Drink 150 g half an hour before meals.
- Liver collection . This collection includes in equal proportions: calendula, immortelle, corn silk, chamomile, string. These herbs not only have a choleretic effect, but also have a positive effect on the liver, intestines, and stomach. The collection is prepared at the rate of 1 tbsp. l. funds for a glass of water. Fill it with boiling water and leave for 1 hour. Strain and divide into several steps.
- Flaxseed oil . It is consumed on an empty stomach, 1 tbsp. l. The product eliminates spasms and improves liver function.
- Fresh juices . An hour after eating, you need to drink a glass of a mixture of carrot, beet and apple juice. This treatment is practiced for at least a month. It is also recommended to mix black radish juice with beet juice and drink 1 glass per day for a month.
- Milk thistle . It is consumed dry or in the form of oil. The product stimulates digestion, reduces inflammation, and stimulates bile secretion.
- Rose hips and nettles . Mix 20 g of rose hips and 10 g of nettle leaves. Pour 250 g of boiling water and simmer in a water bath for 15 minutes. Insist, drink several times a day.
- Honey and mint . Consume 1 tsp three times a day. honey with 3 drops of mint oil. The course of treatment is 1 month.
- Flax with milk . Grind 1 tbsp. flax grains, pour 3 tbsp. fresh milk. Keep on fire until the amount of liquid reduces to the widow. Drink on an empty stomach. The next day, prepare a fresh product. The course of treatment is 10 days.
Prevention of cholestasis
To avoid the occurrence of cholestasis, it is necessary to promptly prevent and treat diseases of the liver and biliary tract, which result in the development of bile stagnation. These include timely removal of tumors and stones. In addition, regular deworming is necessary. You can support digestion processes with the help of herbal preparations, herbal preparations and herbal teas . To prevent bile stagnation, it is necessary to maintain water balance, that is, drink enough clean water. In addition, you need to stop drinking alcohol, which has the most detrimental effect on liver cells, and also adhere to a special diet low in fat.
Markers and laboratory parameters
In cholestasis syndrome, laboratory parameters play an important role in establishing the diagnosis:
- A biochemical blood test will show an increase in total bilirubin due to its direct fraction. This is what gives urine its characteristic dark brown hue.
- GGT (gammaglutamine transferase) serves as a marker of cholestasis when increased threefold.
- An important indicator for this pathology is the level of alkaline phosphatase. Its increase of more than three times indicates an extrahepatic form of cholestasis, and less than three times indicates liver pathology.
- When bile stagnates, the level of lipoproteins and low-density cholesterol increases.
Markers of cholestasis, along with typical symptoms, make it possible to reliably determine not only the presence of stagnation, but also suggest the etiology. But for this research it is advisable to conduct it in the early stages.
Reasons for the development of the disease
All causes of cholestasis can be divided into 2 groups: problems with the production of bile and disruption of the process of its outflow. The main prerequisites for the disease include:
Excessive alcohol consumption, which leads to liver damage and disruption of its functioning.- Viral hepatitis.
- Intoxication of the body with poisons and chemicals. Sometimes such a negative reaction can be provoked by severe food poisoning.
- Liver damage from medications that have a negative effect on the liver.
- Cirrhosis of the liver.
- Blood poisoning (sepsis).
- Malignant tumors in the liver.
- Cholangitis is a disease characterized by inflammation of the walls of the bile ducts.
- Rejection of a transplanted liver or other organs.
- Liver tuberculosis.
- The presence of helminths in the body that affect the liver.
- Sarcoidosis of the liver.
Symptoms of liver cholestasis
Symptoms of cholestasis occur when bile accumulates in the blood and liver tubules. Regardless of the cause of the pathology, there are several common signs:
- discoloration of stool;
- increased liver size;
- digestive problems;
- pain in the right hypochondrium;
- loss of appetite;
- bitter taste in the mouth;
- drowsiness;
- increased irritability.
In 83% of patients, cholestasis occurs against the background of changes in skin color and itching of the epidermis. Unpleasant symptoms intensify in the evening and after meals.
Treatment of hepatic congestion
Before treating cholestasis with conservative and surgical methods, you must consult a gastroenterologist, hepatologist or therapist. Once the cause has been established, only a specialist can offer the necessary assistance tactics.
How to treat?
When symptoms of cholestasis occur, treatment in adults and children is primarily aimed at eliminating the underlying pathology. For this purpose the following is carried out:
- removing or crushing stones;
- deworming;
- tumor excision;
- gallbladder resection;
- drainage of bile ducts;
- anastomosis;
- antiviral therapy for hepatitis;
- cytostatic agents for autoimmune pathologies.
Symptomatic treatment of cholestasis includes taking measures to reduce intoxication, restore and protect liver cells, and improve the outflow of bile. Some improvement in the condition is provided by methods of cleansing the blood of toxins (hemosorption and plasmapheresis). But if the cause of the disorder is not eliminated, then these methods provide only temporary relief.
Drugs
For conservative treatment of cholestasis the following are used:
- products with ursodeoxycholic acid;
- hepatoprotectors;
- antihistamines;
- choleretic (choleretics and cholekinetics);
- vitamins.
For a disease such as cholestasis, drug treatment helps if the outflow disturbance is associated with inflammatory processes. If a mechanical obstruction occurs, surgical intervention must be resorted to.
Diet
The diet for cholestasis is aimed at maximizing the load on the liver. To do this you should:
- eat often and in small portions.
- It is recommended to steam or boil food;
- It is prohibited to use animal fat and fried foods;
- dishes must be warm, hot and cold are prohibited;
- 2-3 hours before bedtime it is useful to consume a low-fat fermented milk product (kefir or yogurt);
- the diet should not contain soda, coffee, alcohol, hot and fatty sauces;
- Do not eat soups containing fatty broths, mushrooms, canned food, chocolate or cocoa.
It is best to steam food for a patient. You need to drink a lot of liquid, at least 1.5-2 liters per day. It is also allowed to use freshly squeezed vegetable and fruit juices, fruit drinks, and compote.
Causes
The principles of treating cholestasis involve eliminating the root cause of bile stagnation, which is why it is important to correctly identify it. Sometimes this takes a lot of time due to the complexity of the secretion production mechanism, as well as the branching of the duct system.
Among the causes of bile stagnation, doctors primarily highlight the following:
- gallstone disease is the most common pathology that provokes cholestasis. The lumen of the duct is blocked by a calculus, the bile ducts expand, and the liver enlarges.
- bending of the gallbladder is usually a congenital phenomenon. There may be deformation in the body, neck or bottom of the organ. Due to deformation, it ceases to perform its functions and becomes a reservoir for the accumulation of bile. The bend is most often accidentally discovered during a preventive ultrasound examination.
- Oncological diseases are a fairly common cause of blockage of the ducts through which secretions from the bladder move. They can contain both a primary tumor and metastases that have grown from the stomach or lungs. In some cases, cholestasis is caused by pancreatic cancer.
- parasitic lesions - as a rule, these are ascariasis and echinococcosis. In the first case, the bile outflow is disrupted by roundworms that have entered the ducts from the digestive organs. In the second, there is a parasitic cyst that compresses the bile ducts.
In addition to the four most common causes of bile stagnation, there are others. These include:
Primary biliary cirrhosis of the liver and its treatment
- alcoholism;
- violation of healthy eating rules and periods of fasting, which can cause temporary stagnation of bile;
- sedentary lifestyle;
- pathologies of the endocrine system;
- diseases of the digestive system;
- impaired motility of the biliary tract;
- infectious diseases;
- sclerosing cholangitis is an autoimmune disease that affects the bile ducts;
- permanent neuro-emotional tension and frequent stress;
- removal of the bladder, which causes bile to accumulate in the ducts, causing inflammation or the formation of stones. In addition, it can enter the intestines in concentrated form;
- changes in hormonal levels during pregnancy;
- congenital pathologies of the muscle tissue of the bladder and ducts;
- long period of taking certain medications;
- metabolic disorder, expressed by pathological changes in the stomach, diabetes mellitus, obesity, atherosclerosis.
Itchy skin is a reason to be wary and have your liver checked