GastrituNet.ru » Stomach diseases
Gastric stenosis - narrowing of its pyloric outlet is a serious pathology that leads to disruption of the digestive process. As a result, disorders of cellular metabolism and disorders of the whole organism develop. Therefore, pyloric stenosis requires timely diagnosis, elimination of its cause and restoration of normal gastric motility.
- 1 Concept of gastric stenosis
- 2 Causes of the disease
- 3 Stages of the disease and general signs
- 4 Features of the course in children
- 5 Diagnostic measures
- 6 Treatment of the disease
- 7 Useful video
- 8 Diet for stenosis
- 9 Prognosis and prevention
Concept of gastric stenosis
The anatomy and physiology of the stomach are such that they provide periodic release of food mass into the duodenum through its narrowed terminal pylorus or pylorus. Its muscles periodically contract, closing the lumen of the stomach, and after a while they relax, allowing the processed food to escape.
What is pyloric stenosis? This is a decrease in its lumen, the width of which is normally at least 1 cm. As a result, the food mass (chyme) is not removed from the stomach in a timely manner, it is delayed, and as a result of stagnation, the processes of its fermentation and rotting develop. As a result, the following pathological processes occur:
- multiplying bacteria and resulting toxic products negatively affect the mucous membrane, causing inflammation;
- in order to push food through a narrowed opening, the stomach contracts intensely, first developing hypertrophy of its muscles, and then atony and an increase in volume;
- Digestion is disrupted, the body does not receive enough nutrients, the function of all systems and organs is disrupted.
Thus, stenosis developing in the pylorus is not only a disease of the stomach, but also affects health in general.
Causes of the disease
According to the international classification of diseases ICD-10, stenosis has a code depending on its cause:
- congenital - Q40.0;
- hypertrophic - K31.1;
- cicatricial - K31.2.
Hypertrophic and cicatricial stenosis are acquired.
Congenital pyloric stenosis
Narrowing of the lumen of the stomach occurs in 1 in 300 newborns and is the result of various developmental anomalies: hypertrophy of the muscle layer, underdevelopment of the nerve plexuses, when a spasm of the constricting muscles occurs.
Hereditary predisposition matters. Provoking factors are infections suffered by the mother during pregnancy, taking antibiotics, sedatives.
Acquired pyloric stenosis
The main reasons for the narrowing of the lumen are:
- peptic ulcer of the stomach and duodenum;
- stomach tumors;
- pancreatic tumors.
In case of a chronic ulcer of the pylorus or duodenum, as a result of repeated scarring, coarse fibrous tissue is formed, which does not allow the pylorus to fully open, and cicatricial stenosis develops.
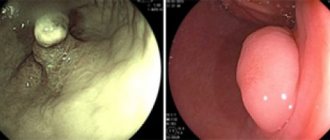
Among tumors, the most common cause of gastric obstruction is cancer growing in the thickness of the wall, less often - tumors growing into the lumen of the stomach, large polyps. Cancer of the head of the pancreas can also compress the stomach and grow into its wall. These types of stenosis are hypertrophic.
Symptoms
Stenosis of the pylorus, located between the stomach and duodenum, has various symptoms that vary depending on the type of disease. The following signs of the disease are distinguished:
- with a compensated type of disease, a slight narrowing of the gastric muscles is observed. The patient feels fullness in the stomach, he often experiences heartburn, to prevent which patients often take soda. In addition, infrequent vomiting brings relief and eliminates discomfort until the next meal. An X-ray examination will help identify acceleration of gastric peristalsis, as well as some slowdown in bowel emptying. Signs of the disease may appear over several years;
- the subcompensated type of the disease is characterized by frequent and profuse vomiting, which relieves the patient of the feeling of fullness in the stomach. Stenosis of the gastric outlet at this stage is already more pronounced. The most characteristic sign of subcompensation is belching of stale (rotten) foods eaten the day before. The patient feels pain in the epigastric region. X-ray shows peristaltic waves from left to right. A sign of the disease at this stage, which can only be determined using an x-ray, is the expansion of the stomach, as well as a violation of its transport function - the contrast agent can remain there for several hours or more than a day. These symptoms of the disease can last about 2 years;
- the decompensated type of the disease represents serious violations of the evacuation function of the gastrointestinal tract. Often decompensation is a symptom of peptic ulcer disease. The patient experiences constant heaviness in the stomach and frequent vomiting. He also feels thirsty due to the constant loss of fluid due to vomiting. In this case, the patient’s skin becomes flabby, and facial features take on a sharp appearance. In the epigastric region, the contours of stretched gastric tissue begin to appear, and the waves of peristalsis disappear. The doctor can easily detect the splashing sound by palpation. X-ray examination reveals a decrease in propulsive function, as well as a large amount of food.
Pyloric stenosis
If the patient constantly vomits, he may lose large amounts of electrolytes, which will lead to a hypochloremic coma.
Stages of the disease and general signs
Acquired narrowing develops gradually as scarring changes in the ulcer or tumor growth increases. There are 3 stages, differing in the degree of obstruction and clinical signs.
- Compensated stenosis , when there is a slight narrowing of the lumen (up to 5 mm), is manifested by belching with a sour taste, periodic vomiting, a feeling of heaviness in the epigastrium, the general condition is not disturbed.
- Subcompensated stenosis, the lumen is narrowed by more than half. The patient has a constant feeling of fullness in the stomach, constant belching and epigastric pain, frequent vomiting after each meal, constipation. The general condition is disturbed: general weakness, pale skin appears, and weight decreases. When palpating the abdomen, a characteristic symptom is determined - “splashing noise” due to a full stomach.
- Decompensated stenosis , the lumen is completely narrowed, food practically does not pass into the intestine. Characterized by constant belching and frequent vomiting with a fetid, stagnant odor, prolonged absence of stool, cramping abdominal pain, constant heartburn due to the reflux of gastric contents into the esophagus. The general condition of the patient is disturbed: exhaustion, anemia, dehydration develops, blood pressure drops, heart rhythm is disturbed, and muscle cramps appear.
Symptoms
Depending on the stage of development of the disease, the manifestations vary. At the initial stage, compensated pyloric stenosis is observed. He is characterized by:
- limited narrowing;
- sour belching;
- feeling of a full stomach after eating.
Vomiting is possible, after which relief occurs for a short period of time. In general, the patient's condition is characterized as satisfactory.
The second stage of development of pyloric stenosis is subcompensation. There are complaints about:
- painful belching;
- vomiting after eating;
- weight loss.
If you seek help from a doctor at this time, a splashing sound can be clearly heard upon palpation in the peri-umbilical area. The final stage of development of stenosis represents the third stage of decompensation:
- the stomach is overly distended;
- there is exhaustion of the body;
- dehydration progresses.
The patient often vomits, but this does not bring relief. The vomit is copious and foul-smelling, and includes the remains of many days' food.
Causes of the disease
Signs of pyloric stenosis are associated primarily with a scar formed from connective tissue. It is formed during the healing of ulcerative lesions of the mucous membrane. The scar tightens the wall of the stomach, which leads to its inactivity. Other reasons include:
- heredity;
- intramural cancer;
- long-term mono-diets, monotonous meals.
As for the hereditary factor, in infants 2-4 weeks after birth, manifestations of congenital pyloric stenosis are detected. An anomaly in the development of the gastric outlet leads to obstruction of patency and difficulty in evacuation of food. The defect is diagnosed 4 times more often in boys.
Intramural cancer develops at almost any age. It affects the stomach tissue and narrows the digestive tract. Food is not transported to the intestines, stagnation processes worsen. Over time, the muscle layer grows, the stomach becomes larger in volume. The process of fermentation and decomposition of food starts.
Which doctor should I contact?
The consequences of the disease are extremely serious. As soon as the first symptoms of pyloric stenosis appear, you should consult a specialist. The solution to this problem is:
Before prescribing treatment, the doctor must draw up the most objective clinical picture possible. To do this he:
- analyzes complaints and manifestations;
- studies anamnesis of illness, lifestyle, family;
- conducts an examination with palpation;
- prescribes laboratory and instrumental tests.
As diagnostic measures, they resort to a general blood test and esophagogastroduodenoscopy. Reliable results are also important:
- radiography;
- electrogastroenterography;
- Ultrasound.
Based on these studies, it is decided what treatment will be: conservative or surgical. After recovery, it is necessary to adhere to preventive measures.
Treatment of pyloric stenosis
Therapy using medications involves a complex effect. Medicines are needed for:
- relief of the main symptoms;
- preparation for surgery;
- adjustments of water-electrolyte and protein balance.
If stenosis is detected at the compensation stage, the doctor prescribes medications intended to relieve inflammation during an ulcer. The subsidence of the process will completely restore patency. In parallel with this, it is necessary to take prokinetic drugs that normalize the motility of the stomach and intestines.
In some cases, endoscopic treatment is used. The narrowed opening between the duodenum and the stomach is expanded with a balloon. The method blocks the functioning of the pyloric valve, while simultaneously restoring patency. This option is not universal and has contraindications. If it is not possible to resort to endoscopic intervention, then open abdominal surgery is performed.
Is surgery necessary?
Unfortunately, quite often the disease is diagnosed in the second and third stages. This cannot be done without the intervention of a surgeon. Important:
- correctly prepare the patient for surgery;
- choose the optimal method;
- completely eliminate the stenosis.
The complexity and duration of the intervention depend on the stage of narrowing, the form of pathology, and the reasons that caused it. Surgery is possible for gastric pyloric stenosis, which involves drainage.
Conservative therapy before surgery is very important, since in most cases the patient’s body is weakened. This is mainly due to the loss of fluid and minerals.
After recovery, it is necessary to visit a gastroenterologist 2 times a year for preventive purposes. If you have complaints about the functioning of the gastrointestinal tract, you should immediately consult a doctor. Meals during treatment and during the rehabilitation period should be fractional. The food is warm; it is not recommended to eat too hot or cold foods or drinks. It is important to limit hot, sour, spicy foods.
Features of the course in children
Congenital pyloric stenosis in children can be acute or have a staged development, but it progresses very quickly. In an acute case, a characteristic symptom is constant regurgitation even after a small amount of feeding, frequent vomiting, disruption of the baby’s general condition - dehydration, lethargy, and there may be muscle cramps. Such children require urgent surgical intervention.
Even with a staged course, congenital pyloric stenosis develops very quickly. In the first days, frequent regurgitation is typical, by the end of the week vomiting occurs, and already in the second week all symptoms are clearly expressed;
- “fountain” vomiting after feeding;
- cheesy appearance and sour smell of vomit;
- white color of vomit without bile;
- decreased urine output;
- constipation, stool is scanty and green in color;
- pale skin, lethargy of the child, the appearance of seizures.
When examining such children, due to the thin and soft abdominal wall, asymmetry is visually determined due to the protrusion of the dilated stomach in the epigastrium. Often, against the background of vomiting, aspiration pneumonia, otitis media and other complications occur - the formation of ulcers, gastric bleeding.
Congenital pyloric stenosis
This disease is usually mentioned separately and coded according to the ICD as Q40.0. It is noted that male children predominate among the patients.
The volume of vomit may exceed the amount of food swallowed.
In newborns, body weight quickly begins to fall, and dehydration appears during the first day.
Treatment of children is only surgical, carried out according to emergency indications after the diagnosis has been clarified using an x-ray examination. After surgery, the recovery period takes 2 weeks.
Diagnostic measures
Additional research methods are used to diagnose pyloric stenosis:
- X-ray;
- gastroscopic;
- ultrasonic;
- functional.
X-ray of the stomach
The study is carried out for adults with barium suspension, for children with water-soluble contrast. Using X-rays, the size and contours of the stomach, the degree of narrowing of the pylorus, the speed and nature of evacuation are determined.
Fibrogastroduodenoscopy
A study with a fiberoptic video probe provides information about the condition of the gastric mucosa, the narrowing and expansion of its lumen, the presence of ulcers, polyps, tumors, and scar changes.
Ultrasound scanning
Allows you to identify the size and condition of the stomach wall - its thickness in various areas.
Electrofunctional study
The electrogastrography method reveals a violation of the motor function of the stomach - the state of its peristalsis on an empty stomach and after eating, to distinguish the stage of compensation from gastric atony with decompensated stenosis.
Diagnosis of the pathological condition
If you notice the symptoms of gastric and duodenal stenosis described above, you should definitely consult a doctor. After the examination, the specialist will prescribe a number of studies, including:
- X-ray examination of the stomach. From the resulting image, you can determine the increase in the size of the organ, as well as the degree of decrease in gastric motility and see the presence of a narrowed lumen between the duodenum. X-rays can also reveal the amount of time it takes for the stomach to move food into the intestines.
- Esophagogastroduodenoscopy. Shows the stage of development of the pathological process, as well as the degree of deformation and narrowing of the lumen between the duodenum and the stomach. In addition, the study will provide information about gastric dilation.
- Study of the motor function of the organ. It is performed using electrogastroenterography and allows you to determine the activity, tone, frequency and nature of peristalsis during meals and on an empty stomach.
- Ultrasonography.
After receiving the examination results and confirming the diagnosis, the doctor prescribes treatment for gastric stenosis.
Treatment of the disease
For stenosis of any stage of the pylorus of the stomach, the only treatment method is surgical - eliminating the narrowing and restoring the passage of gastric contents into the intestine. The choice of surgical method depends on the type and degree of narrowing, the nature of gastric secretion, and the age of the patient. All interventions are divided into 3 groups:
- gastric resection;
- drainage operation - gastrointestinal anastomosis;
- plastic surgery of the pyloric region.
Resection is performed mainly for peptic ulcers with increased secretion; the middle and lower third are removed along with the pyloric region, the remaining upper third of the organ is connected to a loop of the small intestine. They also perform economical resections of only the pyloric region, combining them with vagotomy - the intersection of the branches of the vagus nerves that stimulate the secretion of the glands.
Gastrointestinal bypass is often performed as a palliative (temporarily relieving) operation for inoperable cancer or in elderly patients with heart, respiratory, and kidney failure. It is also combined with vagotomy.
Plastic surgeries are more often performed on children; their options are different, depending on the nature of the anomaly. A typical plastic surgery is when the pylorus is cut lengthwise, then the longitudinal wound is transferred to a transverse position and sutured, thus expanding the lumen.
Modern minimally invasive technologies make it possible to perform operations without large incisions - through a laparoscope and special instruments inserted through small incisions in the skin.
Diet for stenosis
In case of stenosis, the nature of nutrition is of great importance; it must meet the following requirements:
- take food at least 6 times a day in small portions;
- the consistency of the food should be liquid or mushy;
- limit salt, exclude spicy seasonings;
- dishes must be freshly prepared - only boiled, steamed or baked in the oven;
- exclude raw vegetables and fruits, only stewed or baked;
- exclude alcohol, carbonated drinks, sour juices, coffee, black tea;
- food should not be cold or hot, within 30-40°C.
In principle, dietary recommendations for stenosis are not much different from nutrition for peptic ulcers.
Prognosis and prevention
Pyloric stenosis is a progressive disease, so the prognosis is unfavorable for both health and life, especially in children. It must be treated from the moment the first signs appear.
Prevention of stenosis is to a large extent possible in case of peptic ulcer. To do this, you need to constantly adhere to a diet, regularly visit a doctor, undergo examinations and anti-relapse treatment, without waiting for exacerbations. The more often the ulcer worsens and scars, the greater the likelihood of the formation of cicatricial narrowing of the pylorus.