Disease history
A separate section of gastroenterology—pancreatology—is devoted to the study of pancreatitis. The first mention of the pancreas is contained in the works of Aristotle, but a detailed study of the pathological processes associated with this organ was not carried out at that time. The study of the physiology of this part of the digestive system is complicated by its specific location in the body. Significant advances in research occurred at the turn of the nineteenth and twentieth centuries.
The first full-fledged studies were carried out by:
- R.Friz (1889);
- H.Chairi (1886);
- I.L. Dolinsky (1894).
The incidence of chronic pancreatitis increases every year. The risk group began to include men 40-55 years old and children 10-14 years old. Research into the pancreas and pathologies associated with its development continues. Experts are inventing not only new methods for studying patients, but also treatment options for the inflammatory process.
Forms of acute destructive pancreatitis
The disease has three forms, which depend on the intensity of the symptoms and the degree of development:
- Toxemia: toxic substances that have a bacterial environment enter the bloodstream. This form is characterized by nausea, vomiting and diarrhea.
- Abscess. Occurs when pus accumulates in tissues and organs. An abscess can form both in the pancreas itself and in neighboring organs.
- The next form of destructive pancreatitis is purulent changes both in the organ itself and in the retroperitoneal space.
Types of chronic pancreatitis
By origin, chronic pancreatitis can be primary or secondary. In the first case, the disease develops against the background of damage to the gland by a specific factor (alcohol, toxins). In the second, the disease is a complication of other pathological processes (for example, disturbances in the functioning of the digestive organs). According to the severity of the course, CP can be mild, moderate or severe. Chronic pancreatitis always develops with periods of remission and exacerbation.
Features of HP of different forms:
- with a mild course, exacerbations occur once or twice a year (there are no disturbances in the exocrine function of the glands, pain is easily relieved with antispasmodics and analgesics, other signs of CP do not appear);
- with moderate severity, exacerbations become more frequent up to three or four times a year (the exocrine function of the gland is impaired, pain symptoms are more pronounced, the patient may experience a decrease in appetite, weight loss, tests confirm the inflammatory process);
- in severe cases, exacerbations occur on average five or six times a year (the pain syndrome is pronounced, difficult to relieve, body weight decreases to critical levels, diarrhea becomes regular, the clinical picture of the patient’s health is supplemented by most of the symptoms characteristic of CP).
Classification
Additional classification of CP is carried out according to the morphological and clinical picture, as well as clinical manifestations. Determining the specific type of chronic pancreatitis is necessary to prescribe the most effective treatment and make prognoses for the patient.
It is difficult to independently diagnose the form of the disease due to a number of similar symptoms.
Classification:
- according to the morphological picture (obstructive, fibrosclerotic, inflammatory, calcifying);
- according to clinical manifestations (latent, mixed, recurrent, permanent, pseudotumorous);
- according to the functional picture (hypoenzyme, hyperenzyme);
- by the nature of functional deviations (obstructive, hyposecretory, hypersecretory, ductular);
- a separate category includes pancreatic diabetes mellitus (hypoinsulinism, hyperinsulinism).
Symptoms of an attack
Signs of acute pancreatitis may vary depending on the cause of the disease, as well as the severity. If the inflammation is catarrhal in nature, then the symptoms can be tolerated much easier than with purulent lesions of the pancreas.
The main symptoms of acute pancreatitis:
- abdominal pain;
- vomit;
- increased body temperature;
- lack of appetite;
- the appearance of hematomas in the lumbar and abdominal areas;
- yellowing of the skin and mucous membranes.
Pain as the main symptom
Pain in acute pancreatitis occurs suddenly, usually after heavy intake of fatty foods or alcohol. Has a girdling character. Sometimes it occurs in the upper left half of the abdomen, radiating to the spine or stomach area.
The pain is constant and does not go away after taking antispasmodic or painkillers. Always accompanied by nausea or vomiting.
Nausea and vomiting
Nausea and vomiting in acute pancreatitis occur as a manifestation of intoxication syndrome and as irritation of the peritoneal muscles. The nausea is debilitating and ends with vomiting, which does not bring relief.
Vomit may be particles of undigested food and then bile. Vomiting usually does not stop and can lead to dehydration.
Other manifestations
In addition to pain and vomiting, the following symptoms are observed:
- increase in body temperature to 37.5;
- bloating;
- abdominal wall muscle tension;
- facial redness;
- cyanosis of the extremities;
- hematomas in the umbilical region;
- hematomas in the lumbar region;
- increase in abdominal volume.
Causes of the disease
CP is one of the common consequences of gallstone disease and excessive consumption of alcoholic beverages. These factors can disrupt the functioning of the digestive organs in a short period of time (especially in the absence of timely treatment).
With cholelithiasis, the infection enters the gland tissue through the lymphatic system, with bile or through the bile ducts. Alcohol is highly toxic to the pancreatic parenchyma.
Other causes of HP:
- cystic fibrosis;
- genetic predisposition;
- peptic ulcer and its complications;
- autoimmune disorders;
- increased level of calcium ions in the blood;
- uncontrolled use of medications;
- consequences of helminthic lesions of the digestive system;
- complications of atherosclerotic diseases;
- intoxication with harmful substances (ammonia, arsenic);
- complications of pancreatitis of unknown etiology.
Causes
Many causes and predisposing factors to the occurrence of chronic pancreatitis have been identified, among which are: 1. Protein-calorie deficiency. 2. Alcohol and fatty foods. 3. Obstruction of the pancreatic ducts at any level. 4. History of acute pancreatitis. 5. Toxic, including medicinal, effects on the pancreas (organic solvents, cytostatics, furosemide, tetracycline, estrogens, corticosteroids, NSAIDs). 6. Hyperlipidemia. 7. Hypercalcemia. 8. Injuries of the pancreas. 9. Smoking. 10. Antioxidant deficiency. A genetic predisposition to the disease, transmitted by an autosomal dominant type of inheritance, has also been identified.
Symptoms
The first changes in the functional state of the pancreas develop asymptomatically. Disturbances in the functioning of the digestive system are minor and mildly expressed (mild pain that quickly resolves on their own, changes in stool consistency).
From the moment of the first exacerbation of the inflammatory process, the symptoms intensify and are accompanied by painful attacks. The pain may be constant or intermittent.
Symptoms of HP:
paroxysmal pain;- girdle pain;
- pain in the left hypochondrium;
- constant pain in the epigastric zone;
- pain on palpation of the abdomen;
- alternating diarrhea with constipation;
- frequent and debilitating vomiting;
- regular feeling of nausea;
- yellowness of the sclera;
- pallor of the skin.
Features of reactive pancreatitis
Reactive pancreatitis ICD code 10 is a disease characterized by aseptic acute inflammation of the pancreas, which develops as a result of dysfunction of the digestive system or internal organs. After the start of therapeutic therapy, a rapid regression of manifestations occurs. It is primarily characterized by unpleasant pain in the abdominal area, as well as nausea, flatulence, vomiting, fever and signs of intoxication.
To diagnose reactive pancreatitis ICD 10 code in children, a specialist must collect anamnestic data and conduct a physical examination, ultrasound diagnostics, and endoscopy. Treatment is carried out by conservative methods, which includes the use of medications, for example, analgesics, antispasmodics and various enzyme agents. A special diet plays a big role in this, in which there are a number of prohibited foods; they must be excluded from your diet.
Chronic and acute pancreatitis are two dangerous varieties of one serious illness, each of them has a number of features and requires a specific approach. The disease should be diagnosed and treated immediately to prevent the development of complications, some of which can be fatal.
Diagnostic examination
A gastroenterologist diagnoses chronic pancreatitis. After the initial examination, the patient is prescribed laboratory and instrumental examination methods. Deviations in test results will indicate the presence of an inflammatory process. Instrumental techniques will allow you to study the general condition of the pancreas and the digestive system as a whole.
In some cases, patients are recommended to undergo additional examination by specialized specialists.
Laboratory diagnostics
The purpose of laboratory diagnostics is to determine the general health of the patient and identify the inflammatory process. The progression of CP is indicated by increased activity of amylase and lipase, trypsin, elastase and excess fat. Some indicators make it possible to determine enzyme insufficiency of the pancreas before conducting an instrumental examination.
Laboratory diagnostic methods:
- general blood and urine analysis;
- blood biochemistry;
- coprogram;
- stool examination;
- radioimmunoassay.
Instrumental diagnostics
Instrumental diagnostics make it possible to accurately determine the nature of the inflammatory process, the extent of its spread and draw up a clinical picture of the disease. In some cases, several procedures (ultrasound, CT) are performed to confirm the diagnosis. If the process of identifying pathology is complicated by additional factors, then the list of necessary procedures expands.
Instrumental diagnostics:
- Ultrasound of the abdominal organs;
- endoscopic ultrasonography;
- CT or MRI of the pancreas;
- X-ray examination;
- tests with stimulants of secretion or enzyme activity;
- retrograde cholangiopancreatography.
Differential diagnosis
The symptoms of chronic pancreatitis may resemble other pathologies. Differential diagnosis of the inflammatory process should be carried out with a perforated ulcer, intestinal obstruction, acute appendicitis and cholecystitis, as well as intestinal vein thrombosis. In some cases, the manifestations of CP resemble myocardial infarction. This pathology should also be excluded when examining the patient.
Types of pancreatitis according to ICD 10
To systematize and simplify the maintenance of the register of existing diseases, a general classification of diseases was created - the ICD; it is reviewed and, if necessary, redone once every 10 years. This classification is a normative document that is used when assigning a diagnosis to a patient. There are about 40 known classifiers for such a serious disease as pancreatitis; they significantly complicate the relationship between doctors who treat the patient.
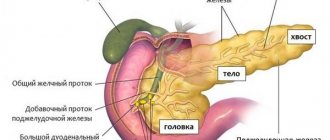
Pancreatitis of the pancreas is often caused by diseases of the abdominal organs
So that specialists from different countries could share their experiences and observations, an international system of diseases was created. Today there is a system of the tenth revision, which is why it is called ICD-10; this classification includes all diseases known to mankind. According to this international registry, ICD 10 pancreatitis is divided into the following types:
- K85 Acute form of pancreatitis.
- K86.0 Pancreatitis of the chronic form of alcoholic etiology.
- K86.1 Chronic pancreatitis of other types.
Each of these forms has a number of features and nuances, which is why it is so important to correctly diagnose the disease before prescribing treatment. To do this, the patient undergoes a series of diagnostic measures, as a result of which the degree of damage to the body, the localization of the inflammatory process, its causes and the form of the disease are determined. Chronic pancreatitis ICD 10, in turn, is divided into 3 main types:
- A calcifying chronic inflammatory process, in most cases this pathology is a consequence of drinking excessive amounts of alcohol. This inflammation changes the structure of the ducts of the affected organ, the process is accompanied by thickening of the secreted fluid, as a result of which the patency of the ducts is impaired.
- Obstructive inflammation of the chronic type can be characterized as a narrowing of the main ducts of the gland or its large branches.
- The inflammatory process in acute form is rare and occurs as a complication of chronic pancreatitis, ICD 10 code in adults.
In some cases, biliary pancreatitis, or as it is called in other sources, bilianodependent pancreatitis, is diagnosed. This disease occurs as a consequence of previously suffered diseases, for example, problems with the liver, biliary tract or gall bladder.
Complication of the disease
Complications of CP are divided into early and systemic. Pancreatitis provokes a violation of the outflow of bile, which can result in obstructive jaundice. Even in the early stages of development, the inflammatory process can cause internal bleeding, infectious complications, abscesses, damage to the biliary tract or phlegmon of the retroperitoneal tissue. These conditions are life-threatening and, in the absence of adequate treatment, pose a threat to life.
Disease progression
CP is a progressive disease. The inflammatory process disrupts the intrasecretory and exocrine functions of the pancreas. The course of the disease has a long-term relapsing nature. In severe cases, a change in the cellular structure of the gland occurs and its functional failure develops.
Systemic complications:
- encephalopathy;
- functional failure of the lungs, liver and kidneys;
- diabetes;
- malignant formations;
- esophageal bleeding;
- critical loss of body weight;
- death.
Treatment
The goal of therapy for chronic pancreatitis is to relieve pain symptoms, maximize the period of remission, and improve the functional parameters of the pancreas. In the absence of effectiveness of conservative and drug treatment, the only way to alleviate the patient’s condition may be surgical intervention. The scale of the operation depends on the stage of development of the inflammatory process and the degree of damage to the digestive system.
Treatment regimen
The treatment regimen for chronic pancreatitis is drawn up individually. Mandatory stages of therapy are taking medications and diet therapy. If treatment occurs using surgical techniques, then the patient’s tendency to recovery will depend on proper rehabilitation.
Rehabilitation therapy is not inferior in importance to basic medical methods.
Approximate treatment plan:
- diet therapy (table No. 5b);
- symptomatic therapy;
- detoxification procedures;
- relief of the inflammatory process;
- restoration of digestive function;
- replacement of pancreatic enzymes;
- surgical intervention (if indicated);
- maintenance and rehabilitation therapy;
- prevention of complications of the inflammatory process;
- regular examination by a gastroenterologist.
Drug treatment
Medicines for the treatment of CP are selected taking into account the individual clinical picture of the patient’s health status. Some of the drugs are recommended for long-term course use. The drug therapy schedule should not be violated. If treatment for CP is stopped earlier than recommended, the period of remission may be shortened.
Examples of medicines:
- enzyme-containing drugs (Pancreatin, Creon);
- analgesics for pain relief (Papaverine, No-Shpa);
- antacids (Maalox, Almagel);
- proton pump inhibitors (Rabeprazole);
- drugs from the group of prokinetics (Cerucal, Motilium);
- anti-inflammatory drugs (Diclofenac);
- drugs to reduce gland secretion (Sandostatin);
- antisecretory drugs (Omeprazole).
Surgery
For patients with CP, surgical treatment is prescribed in rare cases. The main methods of treating pathology of this type are medication and diet therapy. The need for surgery arises when there is no tendency to recovery or serious complications occur. In some cases, emergency surgical procedures are performed to save the patient's life.
Surgical procedure options:
- sanitation and opening of purulent foci (phlegmon, abscesses);
- sphincterotomy (for sphincter blockage);
- pancrectomy (the operation can be complete or partial);
- removal of the gallbladder (if indicated);
- removal of stones from the pancreatic ducts;
- partial gastrectomy;
- creation of circumferential bile outflows (to relieve the load on the pancreatic ducts).
Diet
Diet therapy is one of the main methods of treating CP. If you allow errors in nutrition at any stage of treatment of the inflammatory process, then the tendency to recovery will be significantly reduced. In addition, taking prohibited foods will provoke an attack of pancreatitis. Fried, spicy, salty, fatty foods, marinades, some vegetables (radish, radish), mushrooms, sour fruits and alcoholic drinks should be excluded from the diet.
Allowed to include in the diet:
- lean meats and poultry;
- boiled pureed vegetables;
- steam omelettes;
- vegetarian soups;
- pasta;
- porridge with water or milk;
- fruits with low acidity levels;
- low-fat dairy products;
- low-fat fish (boiled).
When preparing dishes, it is recommended to give preference to the methods of steaming, boiling or stewing. Meals are taken up to six times a day (in small portions). It is important to avoid overeating and starvation. As an addition to diet therapy, you can use medicinal mineral waters (alkaline types of Essentuki, Borjomi).
Sample menu
| Breakfast | Steam omelette, tea or dried fruit compote, oatmeal with blueberries |
| Lunch | Banana (or fruit salad), glass of low-fat yogurt |
| Dinner | Vegetarian soup, boiled turkey with carrots, reduced fat cheese, apple juice |
| Afternoon snack | Baked apple, low-fat cottage cheese |
| Dinner | Rice with lean fish, boiled carrots, whole grain bun, dried fruit compote or tea |
| Before bedtime | Three wheat-oat bread, a glass of skim milk |
Description of the disease
Pancreatitis is an inflammatory disease of the pancreas. The acute form is characterized by attacks of pain, nausea and vomiting. This disease is more often diagnosed in men after 40 years of age and, as a rule, is a consequence of alcohol abuse and long-term dietary errors.
The disease is always severe and painful. For any course of acute pancreatitis, the patient must be hospitalized.
Causes
Alcohol and too fatty foods cause enzymatic hyperactivity of the pancreas, which is the main cause of acute pancreatitis. Other predisposing factors:
- diseases of the gallbladder and its ducts;
- carrying out endoscopic manipulations;
- abdominal surgery;
- taking certain medications;
- congenital anomalies of the structure of the pancreas;
- abdominal trauma;
- viral infections (mumps, Coxsackie virus, herpes viruses, HIV infection);
- autoimmune diseases (systemic lupus erythematosus);
- genetic mutations;
- unbalanced diet;
- liver diseases;
- parasitic diseases;
- pancreatic cancer;
- narrowing of the pancreatic ducts;
- pancreatic cysts;
- hormonal disorders.
Smoking is one of the common factors that can cause damage to pancreatic tissue.
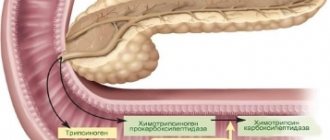
Pathogenesis
The basis of the pathogenesis of acute pancreatitis is aseptic inflammation of the pancreatic tissue, which leads to the release of its enzymes. Substances produced by the pancreas cause intoxication and destruction of organ tissue. They digest pancreatic tissue, causing widespread swelling, damage to its vascular bed, and the development of necrosis.
Forms of the disease
There are two clinical forms of acute pancreatitis:
- edematous;
- necrotic.
In the edematous form, severe inflammation and swelling of the organ develops. Occurs in 80% of cases of the disease. It is characterized by a milder course and is better treated with medications.
In the necrotic form, necrosis, that is, death, of pancreatic tissue occurs. This form is more severe and occurs in 20% of patients with acute pancreatitis.
Classification according to ICD
In the International Classification of Diseases (ICD 10), acute pancreatitis is assigned the code “K 85”.
How to help yourself during an attack of pancreatitis?
If the diagnosis of chronic pancreatitis is confirmed and the patient is able to independently determine the attack, then several recommendations can be used to alleviate the condition. At the first manifestation of CP or too severe pain symptoms, only a qualified specialist can provide proper assistance (you should consult a doctor or call an ambulance).
Algorithm of actions:
- elimination of pain (Paracetamol);
- relief of spasm (Drotaverine, No-Shpa);
- decreased acidity of gastric juice (Omeprazole, Maalox, Phosphalugel);
- decreased pancreatic secretion (Creon, Mezim);
- hunger, cold and rest (you cannot eat food during the day, you can apply a cold compress to the painful area, any stress on the body is excluded).
Prevention
Primary prevention of CP includes standard rules of a balanced diet, a healthy lifestyle and giving up bad habits. If the disease is detected, then after the course of therapy it is necessary to follow all the doctor’s recommendations. Errors in nutrition, excessive physical activity, alcohol and other negative factors will shorten the period of remission and increase the intensity of symptoms of attacks.
Prevention measures:
- quitting smoking and alcohol abuse;
- compliance with the drinking regime (at least one and a half to two liters of water per day);
- limiting the amount of fatty, fried, salty foods in the diet (spicy foods, marinades, spices and seasonings);
- compliance with the rules of a healthy diet (sufficient content of healthy elements and vitamins in the menu);
- balanced diet with the exception of overeating.
Forecast
In CP, the mortality rate reaches 50%. In most cases, the cause of death in patients is complications of the inflammatory process. The development of the disease can be asymptomatic for a long time, but the progression of the pathology does not stop without adequate therapy. In case of CP, the patient should be regularly examined by a gastroenterologist (at least once every six months).
Timely therapy provides:
- persistent and long-term remissions;
- slowing down the inflammatory process;
- reduction of pain symptoms during exacerbation attacks.
Video on the topic: Chronic pancreatitis. What are the symptoms? How to treat? What can and cannot be eaten?
What tests are taken for diagnosis?
A gastroenterologist diagnoses and treats diseases of the pancreas. He conducts a thorough survey of the patient, evaluates his complaints, conducts an examination, palpates the pancreas area, the anterior abdominal wall to assess the degree of tension.
As a rule, an attack of acute pancreatitis is not difficult to diagnose, since the nature of the pain comes to the fore. But to make a more accurate diagnosis, instrumental and laboratory tests are used for acute pancreatitis.
Diagnosis of acute pancreatitis includes the following tests:
- Clinical blood test. It will have increased leukocytes and ESR (indicating an inflammatory process in the body).
- Blood chemistry. Pancreatic enzymes (amylase, lipase) and glucose increase.
- Ultrasound of the pancreas.
- CT scan.
- MRI.
- EFGDS.
- Diagnostic laparoscopy.