What is a neuroendocrine tumor of the pancreas?
Pancreatic neuroendocrine neoplasms (PNEN) are a group of neoplasias (tumors) of different origin, structure and clinical manifestations.
Depending on whether these tumors can secrete hormones and amines, causing carcinoid and other clinical syndromes, they can be classified as functional (F-NEN) or nonfunctional (NF-NEN). Neuroendocrine neoplasms of the pancreas are the most common neuroendocrine tumors.
Most PNENs are low grade but have malignant potential. They grow slowly and remain stable for many years, at least when they are small. However, without treatment, most of these tumors grow and eventually metastasize to the liver.
Pancreatic neoplasms are rare overall: <2% of all pancreatic tumors. Their diagnosis and localization often require significant technology, and their successful treatment requires a thorough multidisciplinary approach.
For these reasons, a patient with a possible or confirmed pancreatic endocrine tumor is best treated in a large multidisciplinary center that includes endocrinologists, gastroenterologists, pancreatic surgeons, and medical oncologists.
APUD system in normal and pathological conditions
The diffuse endocrine system in the form of cells producing hormones and biologically active substances is located in different organs of the body. The greatest severity of the accumulation of cellular structures of the APUD system is presented in the following tissues:
- gastrointestinal tract;
- central and peripheral nervous system;
- bronchopulmonary structures;
- urinary organs;
- endocrine system.
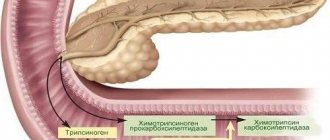
An important organ of the APUD system is the pancreas, whose endocrine cells (islets of Langerhans) produce the following substances:
- insulin;
- glucagon;
- somatostatin;
- pancreastatin;
- cholecystokinin;
- neuropeptides;
- polypeptides.
The vast majority of neuroendocrine neoplasms arise in the pancreatic gland (more than 50%). Much less frequently, apudoms form in the ileum or rectum, in bronchopulmonary tissues, in nerve ganglia and brain structures.
Classification
The term neuroendocrine tumor of the pancreas usually refers to insulinoma, gastrinoma or glucagonoma. Sometimes more rare VIPomas and somatostaniomas are added to this trio.
PNENs are defined as functional or nonfunctional depending on whether they cause a syndrome of hormonal hypersecretion—excessive production of hormones.
Of all functional PNENs, gastrinomas and insulinomas are the most common. Other neoplasias are usually considered together as a group called "rare functional PNENs."
Several such rare clinical syndromes have been proposed as possible functional PNENs. These include the following:
- calcitoninoma;
- parathyrinoma;
- growth hormone-secreting tumor (GRFoma);
- adrenocorticotropin hormone-secreting neoplasia (ACTHoma);
- neurotensinoma.
According to European and American oncologists, non-functional PNEN are more common than functional ones. The former are usually diagnosed in the fourth or fifth decades of life and often have already metastasized to the liver at the time of diagnosis.
Reasons for appearance
10% of functional NENs become a manifestation of hereditary familial endocrine tumors:
- multiple endocrine neoplasia syndrome type 1 (MEN1);
- von Hippel-Lindau disease (VHL);
- neurofibromatosis type 1 (NF-1);
- tuberous sclerosis (TSC).
The reason for the development of these pancreatic neuroendocrine neoplasms is hereditary switching off of the corresponding tumor suppressor gene during fetal development.
Although the outdated term “islet cell tumor” is often used today to identify neoplasms of the endocrine pancreas, it is a misnomer. Many pancreatic neuroendocrine tumors do not develop directly from islet cells.
Most of these neoplasms arise from APUD stem cells. These are the precursor cells from which all types of pancreatic tissue are subsequently formed. They are located in the epithelium of the ducts of this organ.
The fact that many gastrinomas and somatostatinomas are located near the glandular tissue of the pancreas, but not within it, supports the view that these neoplasms may develop extrapancreatically.
Symptoms of the disease
Functional tumors lead to hormonal hypersecretion syndromes.
| Neoplasia | Symptom(s) |
| Insulinoma | Hypoglycemia is a decrease in blood glucose levels. Sweating, weakness, tremors, hunger, etc. |
| Gastrinoma (ulcerogenic pancreatic adenoma) | It manifests itself as a protracted gastric ulcer that is difficult to treat - abdominal pain, nausea, vomiting, etc. |
| VIPoma | Uncontrollable diarrhea, decreased potassium levels in the blood, decreased acidity of gastric juice, dehydration, weight loss. |
| Glucagonoma | Glucose intolerance, dermatitis, stomatitis, glossitis, deep vein thrombosis, depression, heart failure. |
| Somatostatinoma | Symptoms of diabetes mellitus and cholelithiasis, steatorrhea, achlorhydria. |
Nonfunctional neoplasms cause nonspecific symptoms, such as vague abdominal pain, and are usually discovered incidentally.
The distinction between functional and nonfunctional PNEN is based on clinical presentation, and there is no absolute difference in hormone expression between functional and nonfunctional PNEN.
For example, tumor cells in a small PNEN may express glucagon, resulting in borderline elevated glucagon levels. Clinically, however, this PNEN is defined as nonfunctional because a small increase in glucagon is not sufficient to cause glucagonoma syndrome.
Diagnostics
Because recognition of hormonal hypersecretion syndrome requires considerable clinical experience and the symptoms of nonfunctional tumors are nonspecific, the diagnosis of PNEN often occurs quite late.
Endocrine testing, imaging, and histologic findings are essential for accurate diagnosis of PNEN.
A complete diagnosis must establish the nature of PNEN, assess tumor grade, identify primary and metastatic sites, and determine whether the tumor is functioning. If hormonal hypersecretion syndrome is suspected, appropriate biochemical testing is performed to determine it, followed by imaging, endoscopy and biopsy.
If a tumor in the pancreas or liver is incidentally identified by imaging, it is usually biopsied to confirm the presence of PNEN. Biochemical testing is ideally performed even if hormonal hypersecretion syndrome is not obvious, as it may be at a subclinical stage, and hypersecreted hormones can be used as tumor markers during subsequent evaluations.
Diagnosis of the disease
The diagnosis is made using the results of research - laboratory and instrumental.
For endocrine carcinomas, the level of serotonin is determined in the blood and the level of 5-HIAA in the urine. For insulinomas, blood tests are done for the presence of insulin, glucose, C-peptide, and proinsulin. For glucagonomas, a blood test is performed for the presence of glucogen, for gastrinomas, an analysis is done for the presence of gastrin, for VIPomas, an analysis is performed for vasoactive intestinal peptide. In addition, the examination includes:
- scintigraphy;
- PET analysis;
- Ultrasound of the abdominal organs;
- CT and MRI;
- various endoscopic studies.
If there is a suspicion that the tumor is malignant, a biopsy is performed.
Treatment
Patients with pancreatic neuroendocrine neoplasms are treated individually to balance the effects of hormonal hypersecretion. Many pancreatic endocrine tumor syndromes are potentially life-threatening. Therefore, initial medical therapy is aimed at stabilizing the patient's condition to allow a complete preoperative assessment.
All resectable functional or nonfunctional PNEN are recommended to be treated surgically. Different types of surgical intervention are used:
- tumor enucleation (removal of the visible part of the tumor while preserving healthy organ tissue);
- enucleation in combination with pancreatic resection;
- distal pancreatectomy;
- pancreatoduodenectomy (removal of the pancreas and part of the intestine);
- etc.
The type of surgical intervention is determined individually, based on the characteristics of a particular disease in a particular patient. At the same time, neuroendocrine pancreatic cancer requires mandatory excision of lymph nodes.
All resectable insulinomas should be removed surgically, regardless of tumor size. 85–90% of patients with this type of PNEN can be completely cured in this way. Insulinomas account for approximately 35–40% of functional PNENs. Of these, malignant insulinomas account for only about 5–10% of the total.
Systemic therapy is necessary for patients with residual disease after surgery and for the treatment of inoperable tumors.
Synthetic analogues of the hormone somatostatin (growth hormone) are effective against functional PNEN. Their effect is especially pronounced in VIPomas and glucagonomas.
There is no clear evidence that somatostatin analogues treat nonfunctional PNEN, but they are likely to inhibit tumor growth.
Two somatostatin analogues, octreotide and lanreotide, and their long-acting formulations are currently available, and a new analogue, pasireotide, is still in the clinical trial phase with encouraging preliminary results.
Pancreatic cancer: defeating a formidable enemy
What do former King Hussein of Jordan (the richest man on the planet), world-famous founder Steve Jobs (maybe a little less rich, but certainly much more famous), immunologist Ralph Steimann (who died three days before he was awarded the Nobel Prize) have in common? and posthumously creating a precedent - for the first time in history, the prize was awarded to a deceased scientist, as well as to the well-known and beloved actor Oleg Yankovsky, and to many beloved relatives, but unknown to a wide circle of rich and not very rich contemporaries? Much to our regret, the cause of death for all of them had pancreatic cancer.
This is a very serious disease and so far the only effective method of treatment is surgery. Fortunately, not all pancreatic cancers are equally aggressive, which gives a chance of salvation to those who suffer from less aggressive forms.
But this chance can be realized when the attending physician and diagnostician know that only 85-90% of pancreatic cancers are ductal adenocarcinoma, the remaining cancers are less aggressive tumors. And this is already a chance for success. And even ductal carcinoma, if diagnosed at an early stage, can count on long-term survival of patients.
We do not yet know how to form dispensary observation groups for the risk of developing ductal adenocarcinoma (the most common pancreatic cancer), we do not know at what age dispensary examinations should begin, and with what frequency these studies should be carried out. But we have already learned to understand the early signs of pancreatic cancer.
So, if you have performed a tomographic examination of the upper floor of the abdominal cavity, never ignore the pancreas, carefully study all deviations from the norm in the structure of its tissue and in the ductal system. The set of “small” signs allows us to identify early symptoms of pancreatic cancer, and the most important of them is the rupture of the main pancreatic duct for no apparent reason in combination with even moderate manifestations of dystrophy of the distal parts of the pancreas. The second most important sign if you used bolus contrast enhancement is that in the arterial phase you can see a moderately hypodense zone in the gland tissue against the background of unchanged parenchyma intensively accumulating the contrast agent. The cause may be ductal adenocarcinoma, malignancy of an intraductal mucinous tumor, a field of sclerosis with indurative pancreatitis.
Everything revealed in the pancreas should not be “hushed up”, but subjected to critical analysis. Each tomographic symptom has a morphological explanation. And you need to remember, the sooner an explanation for the “strange” is given, the greater the patient’s chances of saving his life.
Intraductal mucinous tumor has already been mentioned above. In English-language literature it is known as IPMN, and the longer it grows, the more likely it is that the N in its name (neoplasia), transforms into a C (carcinoma), which first grows in situ and then transforms into invasive carcinoma. But even the malignant form, intraductal mucinous carcinoma, offers a chance, since it is less aggressive than ductal adenocarcinoma.
Therefore, one must be able to differentiate between IPMNs. They affect the main pancreatic duct, or its lateral branches, or a mixed form is observed. And the most informative study in everyday diagnostic practice will be magnetic resonance cholangiopancreatography.
Segmental sharp expansion of the main pancreatic duct against the background of its remaining unchanged sections, “inexplicable”, similar to a bunch of grapes, cystic expansion of the lateral branches of the pancreatic duct - all this should alert and make one think that such expansion of the ducts is not accidental.
The symptom already mentioned above is the hypodense zone of the tumor in the arterial phase. Contrast enhancement for pancreatic pathology is generally irreplaceable. There is no way without him. It allows you to detect other cancers - neuroendocrine tumors (they are hypervascular), to identify contrasting thin septa in cystic tumors - serous and mucinous cystadenoma (carcinoma). Detect signs of a Franz tumor (the French like to call it that, but we often write and read about it as a solid pseudopapillary tumor), and the larger its size, the more malignant it is. But the smaller it is, the more difficult it is to identify it or differentiate it from the already mentioned neuroendocrine tumor - and here you cannot do without a bolus of contrast enhancement.
Well, when deciding on surgery, there is no way to do without assessing tumor invasion into the great vessels. And here again it is necessary to mention bolus contrast enhancement.
What is the efficiency ratio of tomographic methods? It all depends on the class of devices used. Modern high-field MRI with fast pulse sequences is not inferior to MSCT, and the examination should begin with MRI. T2WI, without and with suppression of the signal from adipose tissue, DWI are effective methods for detecting tumors. Contrast enhancement allows them to be differentiated – in most cases.
A small percentage of “undifferentiated” tumors remains. Traditionally, they resort to a diagnostic puncture. Effective diagnostics. You just need to remember that. a carelessly performed procedure can cause tumor contamination along the puncture channel. Yet non-invasive technologies must dominate.
PET techniques that are fashionable in the West using various radiopharmaceuticals are not always effective and, even in leading clinics in the world, are financially expensive. And not everyone does such research.
What do we have “in the bottom line”? We need to remember about pancreatic cancer, “listen” to our body, to the complaints of loved ones and our patients, and feel like caring trackers when we study tomograms. And always remember - symptoms are not random. In the absence of a system (screening) for pancreatic cancer, only a conscientious diagnostician can save the patient if he does not ignore the early symptoms of the pathology. Be caring and responsible!
Author: Grigory Grigorievich Karmazanovsky Doctor of Medical Sciences, Professor. Head of the Department of Radiation Methods of Diagnostics and Treatment of the Federal State Budgetary Institution Institute of Surgery named after. A.V. Vishnevsky" of the Ministry of Health, member of the European Society of Radiology (ECR), corresponding member of the Radiological Society of North America (RSNA), member of the presidium of the Russian Association of Radiologists (RAR). Laureate of the Russian Government Prize in the field of science and technology. Lecturer at the European School of Radiology.
Progressive treatments for neuroendocrine pancreatic neoplasia in Belgium
In clinics in Belgium, modern methods of minimally invasive surgery, radiation therapy, biological therapy and chemotherapy are used in the treatment of PNEN.
Microinvasive surgical and radiological methods include:
- radioactive polymer microspheres;
- chemoembolization;
- mild embolization;
- radiofrequency ablation (RFA);
- percutaneous alcohol ablation;
- microwave ablation.
Systemic interferon-α2A is used in clinics in Belgium for the treatment of PNEN, which are insensitive to somatostatin analogues.
The mTOR inhibitor everolimus (RAD001) and the tyrosine kinase inhibitor sunitinib are effectively used in Belgian clinics to slow the progression of neoplasia.
Chemotherapy is available for intermediate- and high-grade neoplasias. Temozolomide and capecitabine are the drugs of choice that can be used in patients with rapidly progressing PNEN.
The method of Peptide Receptor Radionuclide Therapy (PRRT) Lutetium Lu 177-dota-tate, developed by Belgian scientists in collaboration with colleagues from the Netherlands, is being successfully introduced into practice. It is effective against well-differentiated PNEN. But this method is not yet widely used, so it is best suited for neoplasias with high malignant potential that are resistant to other systemic treatments
How are neuroendocrine tumors treated?
The following treatment methods are used in the treatment of neuroendocrine tumors:
- surgical intervention;
- chemotherapy;
- biological therapy;
- targeted therapy;
- radiation therapy;
- radiothermal ablation;
- symptomatic therapy.
The radical method of treating this type of tumor is surgical excision within the boundaries of healthy tissue. If the tumor is multiple neoplasms, this type of treatment is not used.
Biological therapy, or immunotherapy, helps the immune system fight the tumor. Substances created artificially or produced by the human body are used to stimulate, reproduce or enhance antitumor immunity.
With the rapid development of malignant neoplasms, treatment with chemotherapy is prescribed. Targeted therapy involves the use of drugs that do not damage healthy cells, but identify cancer cells and destroy only them. Radiation therapy uses large doses of radiation to kill cancer cells. Radiofrequency ablation therapy involves the use of high-frequency electrical current to target tumor sites. To reduce the manifestation of symptoms, symptomatic treatment is carried out using Octreotide and other somatostatin analogues.
The neuroendocrinologist prescribes a treatment regimen for neuroendocrine tumors based on the type, size of the tumor, its location, degree of prevalence and general health of the patient. Combination treatment is often carried out, which shows great effectiveness in treating this type of tumor.
Video on the topic:
Complications
Patients with pancreatic endocrine neoplasia may experience morbidity associated with tumor growth.
- Patients with tumors in the head of the pancreas sometimes have a bile duct blockage, a pancreatic blockage, or both.
- Chronic abdominal pain may occur due to the compressive effect of a large intra-abdominal tumor or obstructive pancreatitis.
Morbidity caused by the effects of excess hormonal production by functional pancreatic neoplasms occurs earlier than the neoplastic effects in the course of the disease.
- If left untreated, patients with insulinoma may experience hypoglycemic seizures and even open coma.
- Before the development of effective antisecretory drugs (eg, H2 blockers and proton pump inhibitors), patients with gastrinoma often experienced life-threatening gastrointestinal bleeding from peptic ulcer disease.
- Patients with VIPomas are at risk of becoming dehydrated from diarrhea. They may also develop fatal cardiac arrhythmias due to associated hypokalemia.
- The morbidity associated with the hormonal effects of glucagonoma can be polymorphic. Patients may have diabetes, malnutrition, stomatitis, and other symptoms similar to severe nutritional deficiencies.
Forecast
The prognosis for most types of PNEN is favorable. But even that neuroendocrine tumor of the pancreas, for which the prognosis is considered good, requires constant monitoring. Because increased growth rate can become an alarming factor that worsens survival.
Because these tumors typically grow slowly and have a relatively low metastatic potential, and because no specific criteria have been defined to predict their behavior, the distinction between benign and malignant neoplasms is based on the presence of metastatic disease.
The five-year survival rate for PNEN without treatment is:
- 80% for all stages;
- 90–100% for localized disease;
- 40% for regional disease;
- 29% for distant metastases.
Long-term disease-specific survival (DSS) of surgically resected tumors exceeds 50% at 20 years.
Because even metastatic pancreatic endocrine neoplasms typically grow slowly, the prognosis of patients with these tumors is relatively good compared with that of patients with nonendocrine cancers.
More than 90% of patients with insulinomas have benign tumors without evidence of metastases, and up to 97% of these patients are completely cured by surgical resection.
Patients with gastrinomas have a worse prognosis. 60% of these tumors are malignant. However, survival rates differ strikingly between patients whose gastrinoma metastases are limited to lymph nodes and those with liver metastases, as follows:
- patients whose gastrinoma metastases involve only lymph nodes may live 25 years or longer, and their life expectancy is indistinguishable from that of people without gastrinoma.
- patients with liver metastases have a 5-year survival rate of 20-30%, compared to 90% for patients without liver metastases.
Approximately half of all VIPomas have metastases at the time of diagnosis or surgery, and approximately one third of patients are completely cured by surgery.
Most somatostatinomas (84%) have already metastasized at the time of presentation, but a number of patients survive 5 years after combined surgery and chemotherapy.
Among endocrine neoplasias, glucagonomas tend to be relatively large (5–10 cm) at diagnosis. In addition, up to 80% of such neoplasias show invasive or metastatic growth. Glucagonoma syndrome is recognized relatively late in most patients, and surgical treatment is possible in less than 20% of all patients. In this regard, such a pancreatic neuroendocrine tumor has the most serious prognosis.
Neuroendocrine tumors: treatment, prognosis, symptoms and classification
Neuroendocrine tumors are the least common type of cancer that develops over several months and arises from the neuroendocrine cells of the body. The danger of this type of cancer: often the tumor is discovered when metastases have already spread.
The reason is that neoplasms develop slowly, without external manifestations until the stage of metastasis, then the disease becomes irreversible. The disease is also called carcinoid (“hidden killer”).
The name is used when the disease affects the bronchi, lungs, and forms neuroendocrine carcinoma.
Often people who develop carcinoids develop a syndrome with the corresponding name. It proceeds as follows: patients experience discomfort in the abdomen, problems with heart valves arise, the respiratory system is disrupted, and diarrhea begins.
In rare cases of an already rare disease (1 patient in 20,000), symptoms have been recorded: ulcers, diabetes, skin and mental problems, weight loss, constant or temporary hunger and seizures. However, the disease is gaining momentum. According to statistics, the number of cases is increasing.
Older patients, predominantly men, are more susceptible to pathology.
It is important to note that depending on the location of the cancer tumor, the disease is dealt with by doctors of the following specializations: gastroenterologist, hepatologist, pulmonologist and others.
The main foundation in which NET development occurs is the neuroendocrine cell. The tumors developing in them have a rare structure and origin, as well as the degree of malignancy. More cells are found in the respiratory organs (25% of cases), gastrointestinal tract (50% of cases), mammary, parathyroid and prostate glands.
So far, scientists have not been able to determine why patients develop the disease. But a popular version related to genetics has been developed. The main factor, according to scientists, is predisposition. Thanks to research in the field of genetics, the appearance of such tumors is explained.
The main symptom of neuroendocrine neoplasms is carcinoid syndrome. The disease develops after the spread of metastases to the liver. Symptoms of the syndrome: problems with the gastrointestinal tract, heart valves, hot flashes, disorders of the respiratory system.
Types of neuroendocrine cancer
If location is taken as the basis for classification, the disease is divided into 2 large groups:
- Bronchopulmonary neuroendocrine tumor. Site of action: bronchi, lungs. Compared to others, this disease occupies three percent.
- Neuroendocrine tumors of the gastrointestinal tract.
Classification of such neoplasms.
- Endocrine carcinomas. They are located in all organs of the digestive system except the pancreas.
- Carcinomas, location - pancreas.
Glucagonoma. In 80% of cases, patients experiencing health problems are diagnosed with this type of neuroendocrine tumor. There are already widespread metastases to the liver or bones, and in rare cases to the lymph nodes and ovaries.
Four out of five cases are considered malignant. More often, the tumor is found by dermatologists, since glucagonoma has a negative effect on the skin. The condition of the dermis worsens: the skin peels off and changes color.
Diabetes mellitus is also recognized as a symptom of the disease.
Vipoma. Rare type of cancer. As practice shows, people with such a diagnosis do not live. The main symptom is diarrhea. It provokes dehydration of the body, removing useful substances.
More often, the tumor forms in the pancreas, lungs, adrenal glands, and the small intestine suffers. Formations can be divided into two groups: pancreatic and extrapancreatic.
In the first case, the tumors often reveal a malignant nature, in the second case - vice versa.
Insulinoma. Because of it, excessive amounts of insulin are released into the body, leading to the development of another disease - hypoglycemia. Location: pancreas. They can be benign and isolated, but sometimes a group of tumors occurs. Women are more likely to develop this type of cancer than men.
Somatostatinoma. Most often, the tumor is located in the pancreas and slightly less often in the duodenum. If in the first case the disease passes in an acute form, many symptoms develop, then in the second case the disease passes noticeably milder.
Gastrinoma. According to the standard, it is located in the pancreas, gall bladder, liver and other places. It activates the abundant secretion of hydrochloric acid, and this, in turn, leads to the development of ulcers in the small intestine. Most often malignant.
Men are predisposed to the appearance of this type of tumor more often than the weaker sex. Often found in patients at the metastatic stage. Gastrinoma spreads in single ulcers. However, a heterogeneous clot can also form.
Scientists in the field of oncology often associate its occurrence with genetics.
How to detect neuroendocrine cancer and go to the hospital on time
The signs that explain that a tumor has arisen are always different. It all depends on the location in the body.
If the site of tumor formation is the organs of the respiratory system, the patient has similar symptoms:
- cough with sputum and blood;
- dyspnea;
- sensations of pain in the chest;
- sudden weight loss;
- refusal to eat.
Once a malignant neoplasm begins to develop, the symptoms will resemble standard bronchitis; it is important to quickly notice the differences.
A growing tumor will cause paralysis of the laryngeal nerve, and this will lead to problems with the functions of the oral cavity.
The behavior of the body when metastases appear is difficult to predict. It depends on the area where the clots spread.
If a gastric neuroendocrine tumor develops, it is classified as a malignant carcinoma.
Symptoms of insulinoma:
- problems with concentration, remembering events;
- headache;
- Difficulty with time orientation.
The cause of pain is an insufficient amount of glucose in the patient’s body. Glucose deficiency is an unpleasant thing. A small amount of the substance can cause unwanted sensations:
- profuse sweating at the slightest physical exertion;
- constantly renewed feeling of hunger;
- trembling in the arms and legs, sometimes leading to convulsions;
- uneven heartbeat.
If neuroendocrine tumors have formed in a patient in the gastrointestinal tract, the patient perceives the consequences:
- regular feeling of heat;
- recurrent diarrhea;
- abdominal pain;
- difficulties with the respiratory system;
- skin problems.
Non-standard manifestations of neuroendocrine formations also occur. For example, spasms in the bronchi, severe tearing, periodic headaches.
If a patient develops somatostatinoma, the patient often experiences negative consequences:
- Fat is also released during stool;
- development of mild diabetes mellitus;
- the occurrence of pain in the abdominal area;
- the likelihood of developing gallstones increases;
- intoxication of the body;
- increased sweating.
If the cause of the cancer is a VIPoma, the patient will have symptoms:
- The emergence of endocrine cholera. This disease is characterized by frequent diarrhea. If the patient constantly eats food, he can lose up to 4 liters of body substances in this state. If a person with this disease does not have a regular diet, the loss will be up to one and a half liters.
- The occurrence of unpleasant sensations in the abdominal area.
- Redness on the skin.
- Mental health problems.
If a patient develops gastrinoma, the following symptoms will appear:
- The occurrence of ulcers that do not respond to appropriate treatment. This can lead to death if bleeding occurs in the gastrointestinal tract.
- Unpleasant sensations in the abdominal area.
- Burning in the chest.
- Body-debilitating diarrhea.
Glucagonoma causes the following symptoms:
- The patient may develop necrolytic migratory erythema of the skin. This disease proceeds like this: redness forms, which turns into spots, then into papules, and finally into unpleasant-looking blisters. Gradually, the blisters burst on their own and skin diseases can occur because of them: eczema, lichen, keratosis, even necrosis.
- Frequent occurrence of oral diseases.
- Complete change in the appearance and color of the tongue.
- The occurrence of diabetes, which occurs in a mild form.
- Sharp weight loss.
Once cancer reaches its peak, location no longer influences patients' symptoms. After the onset of tumor intoxication, patients experience similar things:
- increase in body temperature up to 39 degrees;
- intoxication of the body;
- complete loss of appetite;
- desire to sleep during the day, but lack of this desire at night;
- constant depression;
- increased sweating in the patient;
- in some places the skin turns blue;
- decreased protective properties of the immune system.
Standard symptoms
When considering neuroendocrine tumors, the list shows common signs of NET development in the body, regardless of location.
- Intoxication of the body.
- High blood pressure.
- A sharp reduction or increase in body weight for no good reason.
- Profuse sweating with the slightest exertion.
- Unreasonable feelings of panic or anxiety.
- Irregular heartbeat.
- Regular headaches.
- Rising temperature.
- Red rashes on the skin.
- Lack of appetite.
- Deterioration of vision.
- Gastrointestinal problems.
- Trembling in limbs.
Dangerous deterioration
Sometimes a complication of endocrine tumors occurs - carcinoid crisis. This process can occur against the background of a biopsy, surgery, or severe stress. However, occasionally a situation is possible when deterioration occurs without the influence of external factors, of course.
During this condition, the patient begins to experience severe spasms in the bronchi, a pronounced arrhythmic heartbeat, and blood pressure decreases by an order of magnitude. A carcinoid crisis is deadly for the patient, so if the patient finds himself in this condition, emergency medical attention is required.
Treatment methods for neuroendocrine tumors
Before treatment, the body is diagnosed according to the standard. During it, clinical trials are carried out.
Analyzes
First of all, the concentration of 5-HIAA in the urine and serotonin in the blood is checked. The blood is also checked for the amount of C-peptide, insulin, proinsulin and glucose. If it turns out that the patient has glucagonoma, then they check the presence of the corresponding substance - glycogen; if gastrinoma is suspected, they look at the gastrin content.
Patients suspected of having such diseases should undergo ultrasound, tomography, MRI, MPE and a number of other diagnostic procedures. If there is a possibility that the analyzed tumor is malignant, a biopsy is performed.
Treatment
There are two methods of treating neuroendocrine tumors:
- Operation. This is an effective method for carcionomas. This is where surgery comes into play. Surgeons open the affected area and try to remove any cancer found there. However, it is often not possible to completely remove tumors that have appeared. This is due either to a large number of tumors, or the formations have developed in a secluded place, and it is difficult for surgeons to reach with the help of instruments, or the disease has reached the stage of metastasis, and surgery will no longer help.
- Therapy. If surgery is not available or does not change the situation for the reasons stated above, therapy using somatostatin is performed. When such treatment does not bear fruit or the disease develops too quickly, patients are prescribed serious, dangerous, but effective treatment using chemotherapy drugs.
How do doctors make a prognosis, what is it based on?
Necessary information: the medical prognosis is based on three points:
- level of malignancy of the neoplasm;
- tumor type;
- stage of spread of the disease.
Half of those diagnosed with a neuroendocrine tumor survive five years. A third of people with carcinoid syndrome survive this amount of time, while the rest die earlier. If there is no metastasis process, more than half live at least 5 years after detection of the disease.
If the spread of metastases has occurred, then life continues for the next five years in a third of patients. Glucagonoma has not been sufficiently studied, as it is extremely rare, so the average lifespan of people with this disease is difficult to establish.
But oncologists have produced disappointing information about glucagonoma: a person cannot live with this disease.
How to avoid becoming a victim of a neuroendocrine tumor
It is difficult to give a specific answer, because no working prevention has been developed. Oncology scientists have not invented magic “miracle pills” that help heal or prevent the disease. It is recommended to undergo medical examinations more often: visit a gastroenterologist, perform a blood test, and undergo fluorography.
The only way to reduce the likelihood of neuroendocrine tumors is to quit smoking. According to statistics, in 90% of cases, endocrine tumors are found in heavy smokers. To prevent the occurrence of such oncology and other diseases, it is necessary to lead a healthy lifestyle.
Scientists working in the field of oncology make recommendations to reduce the likelihood of cancer cell development to a minimum, it is necessary to eliminate or mitigate these processes:
- disruption of the immune system and endocrine system;
- being in an environment with external toxic stimuli;
- constant stress;
- bad habits: frequent drinking of alcohol, smoking;
- infectious viral diseases;
- being under the influence of radiation;
- chronic diseases of the gastrointestinal tract.
Source: https://onko.guru/termin/nejroendokrinnye-opuholi.html