Terminology
Achalasia cardia is a disease of neuromuscular etiology and belongs to the chronic form. The disease is characterized by the absence or partial opening of the cardia when swallowing food. Against this background, the patency of the esophagus is disrupted, and chaotic contraction of the smooth muscles of almost all parts of the esophagus develops.
The cardia is a valve, or, in other words, the sphincter of the esophagus. The location of this organ is on the border between the esophagus and the stomach. The main purpose of the sphincter is to regulate food and feces as they move between parts of the body.
If the functioning of the valve is disrupted, then this pathology is called cardia insufficiency, or reflux.
Development mechanism
When the disease occurs, the lower esophageal sphincter stops relaxing during meals. If pressure on the inferior valve increases, the valve narrows further and the esophagus re-expands. As a result, undigested food accumulates.
Most often, the disease develops against the background of pathological changes in the nerve cells located between the walls of the esophagus and the muscle layers. The development of malignant neoplasms and diabetes mellitus can also cause the disease. A possible cause may be dystrophic changes in both muscle fibers and the plexuses of the esophagus, or Chagas syndrome after bedbug bites.
The pathology of achalasia cardia develops quite slowly. The diagnosis can only be made by X-ray examination or endoscopy.
Causes
Gastric cardia insufficiency can occur in any person and at any age. And most often it is not even possible to establish the exact cause of the pathology. And some factors that lead to illness cannot be eliminated from your life. However, there is a certain list of factors that most often lead to achalasia cardia:
- alcohol and tobacco abuse;
- food with a lot of salt;
- excess weight, especially against the backdrop of a sedentary lifestyle;
- irregular meals, snacks before bedtime and “heavy” foods;
- some medicines;
- nervous shocks;
- very rarely the disease can develop during pregnancy.
Diseases that can cause the development of achalasia cardia:
- attacks of suffocation and disturbances in metabolic processes;
- obesity;
- anatomical abnormalities;
- prostration;
- chronic gastrointestinal diseases;
- problems with connective tissues.
Sphincter of Oddi dysfunction (SOD)
The duodenal papilla contains 2 ducts: bile and pancreatic. When the valve spasms, its function is disrupted according to the hyperkinetic type, the outflow of bile and juice in the organ of the digestive system slows down. Spasm of the sphincter of Oddi is a common condition identified by gastroenterologists and is more common in women. It has been noted that among people who have had their gallbladder removed, dyspeptic disorders and abdominal pain are associated with valve dysfunction and occur in 20% of patients.
General functions of the sphincter of Oddi:
- prevent the penetration of intestinal contents into the ducts of the biliary system;
- regulate pressure in the ducts;
- control the process of secretion of pancreatic juice and bile.
The sphincter of Oddi is responsible for the functions and coordinated work of the entire biliary system. When food arrives, during the digestion process, the sphincter begins to contract rhythmically, which is a signal for the opening of the ducts, the release of bile and pancreatic juice. Normally they open almost simultaneously. When there is a spasm and a violation of the synchronicity of the opening of the valves, the secretion of bile slows down, and accordingly, the digestive function is disrupted.
Dysfunction of the sphincter of Oddi is often combined with other diseases affecting the gastrointestinal tract (irritable bowel syndrome).
Stages
Today, there are several stages of pathology development:
- Stage 1. Temporary decrease in sphincter tone, no expansion of the lumen yet.
- Stage 2. The condition is almost the same as at stage 1, but a mild degree of dilatation is gradually developing.
- Stage 3. At this stage of the disease, a stable expansion of the esophagus is already observed with simultaneous suprawall narrowing of the lower part of the esophagus. Scar changes form.
- Stage 4. Achalasia of the cardia at this stage progresses, complicated by fibrous mediastinitis, esophagitis or periesophagitis.
Interesting! GERD - medical history (causes, symptoms and treatment methods)
Individual signs
If gastric cardia insufficiency is diagnosed, doctors distinguish several syndromes:
- Dysphagia syndrome. Clinical manifestations in this case are as follows: a feeling as if there is a “lump” in the chest;
- hard to swallow;
- The patient constantly chokes while eating.
It is easier for the patient to eat solid than liquid food. This is due to the fact that solid foods put a lot of pressure on the pyloric sphincter and promote its opening. Simply put, there is a violation of the passage of food. These symptoms are very important for a correct diagnosis; for example, in the presence of cancer or stenosis, the clinical picture is the opposite, and it is difficult for the patient to eat solid food.
If the cardiac sphincter loses its functionality, then in addition to the syndromes described above, the patient also experiences other symptoms:
- unpleasant odor from the mouth due to changes in the diameter of the valve and the constant retention of food particles in the esophagus. Over time, this can cause erosions and ulcers on the mucous membrane;
- heartburn, the patient feels that the pain is burning and moves from bottom to top;
- some patients even feel how food moves through a valve that does not close, leaving behind a sour taste;
- belching with a sour taste;
- excessive salivation;
- hoarseness in the throat;
- problems with teeth and gums, caries;
- increased heart rate.
This pathology is a progressive condition, so exhaustion and deterioration are increasing.
Features of the cardiac sphincter
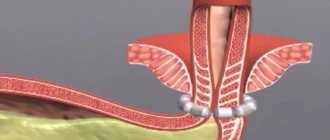
The cardiac sphincter of the stomach ends the tubular part of the upper part of the digestive system - the esophagus. At the same time, the orbicularis muscles mark the beginning of the piriform extension called the stomach. The circular muscles, which make up a transitional anatomical formation, are no more than 1 cm in length. When the circular muscles contract, they do not allow food masses mixed with acidic gastric juice to return to the esophagus. The regulating role of closing and opening is performed by the folded surface of the mucous membrane.
When swallowing a bolus of food, further movement occurs through the esophagus. When the lump approaches the closed barrier valve, it opens and quickly closes. As a result of this mechanism, the reverse movement of food into the esophagus is eliminated. Hydrochloric acid secreted by the lining cells of the stomach causes irritation to the receptors of the esophagus and a burn to the inner surface of the tubular organ. Symptoms of reflux of gastric contents with hydrochloric acid are manifested by burning and heartburn, causing discomfort to the owner.
An angle is formed between the stomach cavity and the esophagus, the value of which is much lower than 90 degrees. There is a direct relationship between reducing the angle and filling the stomach. The degree of tone of smooth muscle circular fibers depends on several parameters:
- deviations from the normal secretion of hormones in the body;
- degree of stretching of the gastric muscles;
- pharmaceuticals;
- the nature of the food consumed (flour, salty, sour, fast food);
- pressure created in the abdominal cavity;
- frequent, severe cough;
- severe tension in the abdominal muscles.
Possible complications
Most often, if sphincter insufficiency is present, gastroesophageal reflux and esophageal stricture subsequently develop.
Lack of treatment can lead to the development of cancer, the statistics in this case are disappointing - from 2% to 7%.
It is also possible as a complication the appearance of megaesophagus, that is, a dramatic increase in the width of the size of the esophagus. This diagnosis is made in approximately 20% of patients.
Interesting! GERD: causes and clinical manifestations
Diagnosis methods
The main goal of diagnosis is not only to confirm or refute cardiac spasm, but also to exclude the presence of cancer in the stomach.
As a rule, laboratory tests do not provide any information at all, which is why they are used to determine concomitant pathology.
To determine how the upper and lower esophageal sphincters work, first of all, X-ray examination is used. Diagnosis is carried out with a barium element, which is injected into the stomach on an empty stomach to determine whether the lower valve is closed, which is typical for this type of pathology. The shape of the esophagus may take on something similar to a "bird's beak". The lower esophageal sphincter is usually unchanged in size, and fluid accumulation can be seen above it. At an advanced stage, the esophagus takes on an S-shape.
To clarify the diagnosis of esophageal achalasia and identify the degree of damage to the mucous membrane, and to refute or confirm cancer, esophagoscopy is used. This study is also a preparatory stage in preparation for surgery.
Manometry is designed to assess the degree of contractile activity and the development of achalasia of the cardia, the work of peristalsis.
Diagnostics
Gastroenterologists are involved in identifying and treating the disease. Dyskinesia of the mixed, biliary type is established on the basis of complaints and data from laboratory and instrumental diagnostic methods. More often, people complain of pain in the right hypochondrium, its intensification after eating and frequent occurrence at night. According to the results of laboratory tests, an increase in the level of bilirubin, amylase, and transaminases is noted in the blood.
A characteristic sign of spasm of the sphincter of Oddi is the absence of symptoms of the inflammatory process, which is noted in acute cholecystitis and pancreatitis. Urine examination reveals no abnormalities. Laboratory test data during and after an attack are different, that is, some indicators outside an attack are within normal limits.
Instrumental diagnostic methods:
- Ultrasound of the biliary tract and liver. The main way to make a diagnosis. During the study, it is possible to distinguish dysfunction of the sphincter from hyperkinetic dysfunction of the gallbladder, and carry out differential diagnosis with other diseases. During ultrasound, provocative tests are used, before and after them the size of the common duct of the gallbladder is determined.
- Hepatobiliary scintigraphy. Radioisotope research method. Drugs are injected into the blood, enter the liver and are excreted in bile. If the function of the sphincter is impaired, their removal slows down.
- Manometry of the sphincter of Oddi is an endoscopic study that provides information about the pressure in the valve, common bile duct, and duodenum.
- Endoscopic retrograde cholangiopancreaticography. Used to exclude pancreatitis, sphincter compression, and the presence of stones in the common bile duct.
Treatment
To reduce the severity of symptoms and eliminate any obstacles that may occur during the passage of food, 3 treatment methods are used:
- treatment with pharmaceuticals;
- non-drug therapy;
- surgical intervention.
Conservative
The main criterion for the effectiveness of drug treatment is the elimination of symptoms. To determine the effect experimentally, an X-ray examination is carried out with parallel administration of barium. If barium suspensions pass normally through the esophagus, then the treatment has helped.
The following are used in therapy:
- nitrates and calcium channel blockers, which reduce lower esophageal sphincter pressure;
- sedatives.
Psychotherapy is usually recommended to patients along with medications.
Non-drug and surgical
The effect of such treatment is possible mainly in the first stage of the disease. In this case, diet therapy is used, which requires eating in small portions, chewing food thoroughly. After a meal, be sure to drink water, which should wash away food debris from the esophagus. Food should be cooked gently and be neutral in temperature.
Pneumatic cardiodilation for esophageal achalasia consists of dilation of the inferior valve while simultaneously delivering air or fluid under high pressure. In practice, it looks like this: a balloon is inserted into the esophagus under fluoroscopic control. Once the balloon reaches the diaphragm, it is inflated. The treatment method is effective in 75% of cases, but there is a high risk of a side effect in the form of GERD.
Endoscopic cardiodilation is recommended for significant curvature of the esophagus. However, the technique also has a side effect - gastric perforation, which occurs in 5% of cases.
If the patient is not recommended for expansion of the esophageal valve, surgery, or the patient is elderly, then chemical denervation is performed. The effect is achieved in approximately 80% of cases and can last up to 12 months. The essence of the technique is that ethanolamine oleate or botulinum toxin is injected into the esophageal sphincter using an endoscopic needle.
Cardiomyatomy is used if previous procedures to widen the valve have not helped. But there is a huge risk that reflux or strictures will appear - this happens in 15% of cases. The essence of the technique is that after the introduction of anesthesia, local or general, a gradual expansion of the passage is carried out with cylinders of different diameters. The procedure is short-term, no more than 2 minutes. Between procedures (on average 5-6 will be required) a minimum of 4 days should pass.
Interesting! Classification of GERD by ICD 10 code and other parameters
The pathology of gastric cardia insufficiency can be treated using partial fundoplication. The procedure is also recommended for cicatricial changes on the walls of the esophagus. Treatment consists of cutting the membrane near the junction from the stomach to the esophagus. After cutting, the edges of the incision are sutured to the fundus of the stomach. The operation requires a recovery period of about 14 days, which will most likely have to be spent in the hospital, but in any case without going to work.
Good results can be achieved by using natural remedies. You can prepare a decoction of anise and fennel, which perfectly relieve inflammatory processes occurring on the mucous membrane. To get rid of heartburn and pain, you can use raspberry leaves or make chamomile or mint tea. However, it should be remembered that before using folk remedies, it is better to consult a doctor so that he can help you select doses taking into account damage to the mucous membrane.
If none of the recommended and carried out methods produces results, then an operation is performed to remove the esophagus.
Physiological regulation of the pyloric sphincter
A complex network of physiological signals controls the opening and closing of the pyloric sphincter. These signals come from either the stomach or duodenum.
Gastric factors
1. There is a group of cells in the fundus that generate a constant fundamental electrical rhythm (BER), which consists of slow depolarizations that move throughout the stomach. During digestion, these basic electrical rhythmic waves are able to excite action potentials in smooth muscle and cause strong peristaltic waves to mix food and gastric juices. The waves push the partially digested food toward the pylorus and force the pyloric sphincter to open to allow a few milliliters of chyme to pass through at a time.
2. The volume of food in the stomach also affects the pyloric sphincter. When there is a large volume, it stretches the walls of the stomach, which in turn creates strong peristaltic waves and prevents the sudden closure of the pyloric sphincter, allowing large volumes of chyme to penetrate the duodenum.
3. Certain foods cause the release of certain hormones, which increases the rate at which the stomach empties. Meat promotes the release of gastrin from the gastric mucosa, which accelerates the opening of the pyloric sphincter. Foods rich in carbohydrates speed up the gastric emptying process, while foods rich in proteins contribute to a much slower rate, and foods high in fat are the slowest.
4. The pH of chyme is also another regulating factor. When acidity increases in the stomach, the pyloric sphincter opens, and when acidic contents enter the duodenum, acidity levels increase and cause the sphincter to immediately close.
5. The increased osmotic pressure in the stomach also causes the expulsion of chyme into the duodenum.
Duodenal factor
1. High acidity and high levels of fat or protein in the duodenum cause the enterogastric reflex, which travels through the duodenal wall through the nerves and promotes the closure of the pyloric sphincter to stop the entry of chyme.
2. Enterogastrons also affect the activity of the pyloric sphincter. These are hormones that help close the sphincter and reduce stomach churning. Cholecystokinin (CCK) is released when fat levels are high in the duodenum and inhibits the gastrin releasing effect in the stomach. Another hormone called gastric inhibitory peptide (GIP) can also affect it in the same way, but to a lesser extent.
Methods for strengthening the lower valve
As a rule, patients are offered all treatment methods. In our country, alternative methods of strengthening the sphincter are not widely used, although world practice proves their high effectiveness.
There are breathing exercises for gastric cardia insufficiency that allow you to get rid of symptoms in the first stages of achalasia. Therapeutic exercises must be carried out on an empty stomach, using abdominal and chest breathing.
Restoration of the sphincter can be carried out with the help of physical therapy. Treatment is best carried out against the background of conservative therapy, even in the acute period. Electrophoresis and DDT are usually used. Naturally, it won’t work directly on the valve, but the phrenic nerve is stimulated with current. The procedures are carried out about 10 times, every other day.
The electrophoresis method is similar, but medications are applied to the cuff with electrodes. The therapy allows for improved blood supply and healing occurs much faster. Some patients note a slight decrease in pain.
How to strengthen the esophageal sphincter?
In addition to surgical methods, the functioning of a low esophageal valve can be restored using physiotherapeutic procedures. Physiologists have approached this problem in a comprehensive manner: they act on the esophageal canal and nearby organs with currents of various frequencies. The following have shown themselves to be effective:
- diadynamic currents ( DDT );
- drug electrophoresis.
These procedures can be performed in conjunction with the insertion of an internal probe. Thus, microcirculation of the organ increases, healing proceeds better, and a mild analgesic effect is noted. This way, without intervention, the integrity of the esophageal organ is restored and the tone of the cardiac valve is strengthened.
Forecast
If the disease is at stage 1, then the prognosis is quite favorable. Especially if the patient strictly follows the doctor’s recommendations. Physiotherapy and breathing exercises will help restore the sphincter.
The second and third stages are no longer the best prognosis for the patient’s recovery. Most often it is not possible to do without surgical intervention. Patients at this stage after treatment will have to be regularly examined to avoid exacerbations.
If left untreated, esophageal achalasia leads to carcinoma in approximately 5% of cases, and aspiration pneumonia occurs in 10% of cases. Patients will have to give up irregular meals and heavy physical work.
Prevention of sphincter of Oddi dysfunction
There are no specific preventive measures aimed at this disease. You just have to follow the general rules that reduce the likelihood of developing gastrointestinal diseases:
- eat rationally, include fruits, vegetables, cereals in your diet;
- do not abuse alcoholic beverages;
- stop smoking;
- maintain an active lifestyle;
- Avoid stressful situations whenever possible;
- do not abuse carbohydrate, fatty foods, and especially fast foods.
For the purpose of early detection of diseases and their treatment, including those of the gastrointestinal tract, undergo preventive examinations.
With timely treatment, signs of the disease in adults and children in 90% of cases disappear within a few days. If you seek medical help late, conservative therapy is ineffective. In addition, frequent exacerbations lead to the development of complications in the form of pancreatitis, gastroduodenitis, cholelithiasis and other diseases of the gastrointestinal tract.