General information
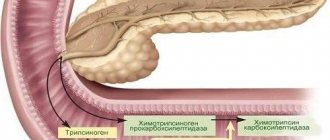
The pancreas is an organ of the human digestive system that simultaneously performs an exocrine function (secretes digestive enzymes) and an intrasecretory function (synthesis of hormones - insulin , glucagon , somatostatin , pancreatic peptide ). Malignant tumors of this organ can be localized in the endocrine and exocrine sections, as well as in the epithelium of the ducts, lymphatic and connective tissue. The ICD-10 code for pancreatic cancer is C25. Anatomically, the gland consists of parts - head, body, tail. The subheadings of ICD-10 include processes localized in various departments and have codes from C25.0 to C25.8. If we consider the anatomical localization of the tumor process, then more than 70% of all malignant tumors of the gland occur in the head. This is a disease of the elderly - its greatest incidence is at the age of 60-80 years and very rarely at the age of 40 years. Men get sick 1.5 times more often. The disease is more common in people who eat high-carbohydrate and fatty foods. In patients with diabetes, the risk of developing this disease doubles.
Pancreatic cancer remains the most aggressive and is characterized by extremely low patient survival. This is due to the fact that the malignant tumor is asymptomatic, difficult to diagnose and early metastasizes to the lymph nodes, lungs and liver, and also quickly spreads through the perineural spaces and grows into the duodenum and colon, stomach and large vessels. In 52% of patients, it is detected in late stages - at the time of diagnosis there are already liver metastases. Early diagnosis is often an impossible task. Even with regular ultrasound, it is not always possible to detect cancer at an early stage.
Over the past 40 years, there have been few advances in diagnosis and treatment that would improve this situation. Despite the improvement of the surgical method and the performance of extended operations, they do not show benefits at those stages at which this disease is detected. Despite its rare occurrence (compared to malignant diseases of other locations - lung, stomach, prostate, colon and breast), mortality from pancreatic cancer ranks fourth in the world. In this regard, research is aimed at finding methods for early diagnosis and the most effective chemotherapy .
Therapeutic measures
The only treatment for pancreatic tumors is surgery. There is no way to remove the tumor with medications yet. If the neoplasm is benign, then surgical intervention will allow the patient to be completely cured, and he will be able to continue to lead a normal life. In addition, medications may be prescribed to reduce the intensity of symptoms, as well as a special diet.
A malignant tumor has a more unfavorable prognosis. Due to the fact that it is usually detected in late stages, a person may not be taken for surgery, since the tumor will either grow into other organs or metastasize. Therapy is aimed at maintaining a person’s life. For this purpose, radiation and chemotherapy, narcotic analgesics are prescribed.
Pathogenesis
It is known that chronic pancreatitis increases the risk of pancreatic cancer by 9-15 times. The main role in the development of pancreatitis and cancer belongs to the stellate cells of the gland, which form fibrosis and at the same time stimulate tumorigenesis. Stellate cells, producing extracellular matrix , activate the destruction of gland cells and reduce insulin production by β-cells. At the same time, they increase the oncogenetic properties of stem cells, stimulating the occurrence of pancreatic cancer. And the constant activation of stellate cells disrupts the homeostasis of the tissues surrounding the tumor, which creates the ground for the invasion of cancer cells into neighboring organs and tissues.
Another factor in oncogenesis is obesity . Obesity undoubtedly affects the pancreas. Visceral fat is an active endocrine organ that produces adipocytokines . In insulin resistance, steatosis and inflammatory cytokines cause organ dysfunction. Elevated levels of free fatty acids cause inflammation, ischemia , organ fibrosis , and ultimately cancer .
The following sequence of changes in the pancreas has been proven - non-alcoholic steatosis , then chronic pancreatitis and cancer . Patients quickly develop cachexia , which is associated with dysregulation of the hormones ghrelin and leptin under the influence of the same cytokines. If we take into account gene mutations, it can take 10 years from the appearance of the first signs of mutations to the formation of a non-invasive tumor; then it takes 5 years for the transformation of a non-invasive tumor into an invasive one and the development of a metastatic form. And after this, the oncological process quickly progresses, leading to an unfavorable outcome within 1.5-2 years.
Classification of pancreatic tumors
All gland tumors are divided into epithelial (they make up 95%) and neuroendocrine (5%). Epithelial tumors, in turn, are:
- Benign (rare). These include: serous and mucinous cystadenoma , mature teratoma and intraductal adenoma .
- Borderline (rarely diagnosed, but have malignant potential). These include: mucinous cystadenoma with dysplasia , solid pseudopapillary tumor and intraductal tumor with moderate dysplasia .
- Malignant.
Malignant ones include:
- Serous and mucinous cystadenocarcinomas .
- Ductal adenocarcinomas .
- Pancreatoblastoma.
- Acinar cell carcinoma.
- Mixed cell adenocarcinoma.
- Intraductal papillary mucinous carcinoma.
The most common malignant tumor is ductal adenocarcinoma, which is a highly aggressive tumor. Carcinoma in 75% of cases develops in the head. The remaining cases are in the body and tail.
Cancer of the head of the pancreas in 83% of patients has characteristic symptoms - jaundice and itching. Moreover, half of the patients present with end-stage jaundice, which is often combined with signs of duodenal obstruction. Depending on the stage, radical surgery to remove the tumor may be performed. It is performed if the tumor diameter is no more than 2 cm. But even after radical operations, survival over the next 5 years is observed in only 3-5% of patients. Surgery alone does not provide good results, so it is supplemented with chemoradiotherapy , which increases survival.
Palliative operations, which are designed to alleviate the condition with the possibility of radical treatment, are performed for locally advanced unresectable head cancer and involve the formation of various types of anastomoses . The main criteria for unresectable tumor of the head are its connection with the mesenteric vessels, invasion into the celiac trunk and the hepatic artery. In elderly people in the presence of stages III–IV, the least traumatic operation is performed - cholecystogastrostomy .
Stages of pancreatic cancer
- Stage IA: T1 (at an early stage, the tumor is within the gland up to 2 cm in size, that is, the tumor can be detected), N0 (no regional metastases), M0 (no distant metastases).
- Stage IB: T2 (tumor of the head within the gland, but larger than 2 cm), N0 (no regional metastases) M0 (no distant metastases).
- Stage IIA: T3 (tumor outside the gland: has spread to the duodenum, bile duct, portal vein, but the mesenteric artery is not involved), N0, M0 - no regional or distant metastases. The tumor is operable, but in 80% of patients there is a relapse after surgery.
- Stage IIB: T1-3 (tumor size and distribution may be the same as in previous stages, N1 (metastases in regional lymph nodes), M0 (no distant metastases).
- Stage III: T4 (tumor spread to the celiac trunk and superior mesenteric artery), any N, and no distant metastases - M0.
- Pancreatic cancer stage 4 - any tumor, any N and distant metastases - M1. Surgery is not indicated; other treatment methods are used.
Benign formations include:
- Serous cystadenomas , which have a minimal risk of malignancy, very slow growth, are located in any part of the gland and very rarely communicate with the duct. This type of benign tumor is diagnosed in women 50-70 years old.
- Retention cysts and pseudocysts . Both varieties occur after 45-60 years. If retention cysts are located in the head of the gland, then pseudocysts are characterized by localization in the body and tail.
- Solid pseudopapillary tumors are rare, localized anywhere in the gland, rarely communicate with the duct, and develop in young women 20-40 years old.
Among benign tumors, adenoma is the most common. There are the following histological variants:
- acinar - its structure resembles exocrine glands;
- neuroendocrine;
- ductal - comes from the epithelium of the ducts.
Acinar adenoma is morphologically reminiscent of acinar cells that produce pancreatic enzymes.
It consists of cysts of various sizes, is very rare and is most often localized in the head, much less often - in the body and tail. The size of these tumors can range from millimeters to 10-20 cm. More often they are asymptomatic. Despite its significant size, the patient's general condition remains satisfactory. Only large adenomas compress nearby organs and can be felt through the abdominal wall. When the pancreatic and bile ducts are compressed pancreatitis , jaundice , and cholangitis . If the tumor is hormonally active, clinical manifestations will depend on the secretion of one or another hormone. The tumor is detected by ultrasound and computed tomography.
Neuroendocrine tumor occurs in only 2% of cases. As a result of research, one in five people with a neuroendocrine tumor is identified as having a genetic predisposition to cancer, since these tumors contain a large proportion of germline mutations. Patients with such tumors have a better prognosis, however, these tumors are unstable - slow growth and rapid metastasis are possible.
Some types of cysts are very prone to malignancy and are classified as borderline. Thus, mucinous cystic formations and intraductal papillary mucinous formations are considered as precancerous conditions. The latter are most often localized in the head and are found in elderly people. What signs most often indicate malignancy?
- the presence of parietal nodes in the gland;
- cyst size is more than 3 cm;
- dilatation of the main pancreatic duct.
Separately, it is worth highlighting gastrinoma - it is a benign endocrine gastrin-producing tumor, which in 80-90% of cases is located in the pancreas or the wall of the duodenum. The possibility of localization in the peritoneum, stomach, hilum of the spleen, lymph nodes or ovary cannot be excluded. Its manifestation is Zollinger Ellison syndrome - increased secretion of gastric juice, development of aggressive peptic ulcers in the duodenal bulb, perforation, bleeding, stenosis.
The first manifestation of Zollinger Ellison's sign is diarrhea . The biochemical indicator of this syndrome is the level of gastrin in the blood. Normally, its level is 150 pg/ml, and with this syndrome it is more than 1000 pg/ml. of hydrochloric acid is also determined . For isolated gastrinomas, tumor resection is performed. But even after resection, remission within 5 years occurs in only 30% of patients. In 70% of patients, it is impossible to completely remove gastrinoma, so such patients undergo massive continuous antisecretory therapy. In 2/3 of cases, gastrinomas are malignant, but grow slowly. Metastasizes to regional lymph nodes, liver, peritoneum, bones, skin, spleen, mediastinum.
Symptoms and course of cancer of the body and tail of the pancreas
The clinical symptoms of cancer of the body and tail of the pancreas are significantly different from the symptoms of cancer of the head. When the body or tail is affected, the common bile duct, portal vein, and also part of the Wirsungian duct from the neoplasm to the duodenum are not involved in the process. Therefore, no jaundice, discolored or fatty stools are observed; ascites can appear only in late stages with metastases in the abdominal cavity. But damage to the middle part, as a rule, causes extremely severe pain in the depths of the epigastrium due to the proximity of the solar plexus. These pains are constant in some cases, intermittent in others, and often reach extreme intensity. Once they appear, they do not leave the patient until death; radiate to the left hypochondrium, into the space between the shoulder blades. They intensify from movements, from eating and are somewhat weakened by bending the body forward, since in this position the pancreas and cancerous tumor put less pressure on the aorta and solar plexus.
A tumor of the gland body, if palpable, usually transmits pulsation of the aorta. By compressing the splenic vein, body tumors sometimes cause swelling of the spleen. Tumors of the body and tail of the pancreas easily spread to the posterior wall of the stomach and the greater curvature, causing corresponding stomach symptoms. From the tail, cancer can spread to the retroperitoneal tissue, adrenal gland and kidney.
Causes
The exact reasons have not been identified, but there is evidence of the role of certain factors:
- Diseases of the pancreas. First of all, chronic pancreatitis . In patients with alcoholic pancreatitis, the risk of malignant diseases of the organ increases 15 times, and with simple pancreatitis - 5 times. With hereditary pancreatitis, the risk of cancer is 40% higher.
- Pancreatic cysts, which in 20% of cases develop into cancer. A high risk of malignancy is indicated by a family history of cancer of this organ.
- Genetic mutations. More than 63 mutations are known to lead to this disease. 50-95% of patients with adenocarcinomas have mutations in the KRAS2, CDKN2 gene; TP53, Smad4. In patients with chronic pancreatitis - in the TP16 gene.
- Obesity , which is always associated with pancreatitis , diabetes and an increased risk of prostate cancer. Obesity during adolescence increases the risk of cancer in the future.
- Type of food. A diet high in protein and fat, lack of vitamins A and C, carcinogens in food (nitrites and nitrates). An increased content of nitrates in products leads to the formation of nitrosamines , and they are carcinogens. Moreover, dietary habits and the carcinogenic effects of foods appear after several decades. Thus, nutritional characteristics in childhood and young adulthood also matter.
- Increased levels of cytokines (in particular IL-6 cytokine), which play a role not only in the development of inflammation, but also in carcinogenesis.
- Smoking is a proven risk factor for cancer of this organ.
- Exposure to ionizing radiation and carcinogenic fumes (for example, in the aluminum industry, dry cleaners, oil refineries, gas stations, dyeing industries). These unfavorable environmental factors cause DNA changes and failure of cell division.
- Gastrectomy (removal of the stomach) or gastric resection. These operations for ulcers and benign tumors of the stomach increase the risk of pancreatic cancer several times. This is explained by the fact that the stomach is involved in the degradation of carcinogenic substances entering the body with food. The second reason is the synthesis of cholecystokinin and gastrin in the mucosa of the small intestine and pylorus (due to the absence of the stomach or part of it), and this stimulates hypersecretion of pancreatic juice and disrupts the normal functioning of this organ.
Diagnosis and staging
The diagnosis is based on anamnestic data, the result of examination and additional research methods.
The latter include laboratory and instrumental diagnostics.
The patient's complaints such as abdominal pain, rapid weight loss, changes in general health for the worse, vomiting, nausea and other classic signs of the disease are taken into account.
A visual examination reveals yellowness of the skin, mucous membranes, haggard appearance, and pallor.
To confirm/refute the cancer process, instrumental diagnostic methods are used:
- Ultrasound. Echography involves a thorough examination of all internal organs located in the peritoneal cavity and in the space behind it. The key to the informativeness of the method is proper preparation for the study. The organ is located deep and difficult to see. If there is an accumulation of gases in the intestines or food debris in the digestive canal, it can be difficult to examine the parenchymal tissues of the organ.
- Tomography. From this category of research methods used to diagnose pancreatic cancer: MRI (magnetic resonance imaging )
- CT (computed tomography) . The first of them is considered more informative. With its help, you can reliably visualize parenchyma tissue, determine the degree of development (stage) and structure of the neoplasm.
Symptoms of pancreatic cancer
The first signs of a pancreatic tumor are difficult to determine, since at an early stage the process does not manifest itself and proceeds hidden. The presence of clinical symptoms means that the process is already widespread. At the time of diagnosis of the disease, 65% of patients have metastases to the liver, lymph nodes (in 22% of patients) and lungs. However, it is worth paying attention to the nonspecific first symptoms of pancreatic cancer at an early stage - fatigue, fatigue, changes in bowel function ( constipation or diarrhea ), periodic nausea. Further symptoms depend on the location of the tumor in the gland - the predominance of certain symptoms makes it possible to suspect one or another location of the tumor.
A malignant tumor of the head of the pancreas manifests itself as jaundice and itching. However, manifestations in the form of jaundice and itching are not early symptoms of the disease. Jaundice discoloration of the skin appears in complete well-being and without pain symptoms. Only in some patients jaundice is accompanied by abdominal pain or discomfort. Jaundice in glans cancer is due to the fact that carcinoma , increasing in size, spreads to the bile ducts, and compresses their lumen and the lumen of the duodenum, into which the common bile duct flows.
Jaundice may be the first and only symptom in some patients. It is of an increasing nature and its intensity depends on the size of the tumor. The jaundiced color of the skin gives way to olive, then dark green. Yellowness of the sclera and mucous membranes of the oral cavity is also characteristic. A decrease or complete cessation of the flow of bile into the intestines causes the appearance of colorless feces and the development of dyspeptic symptoms (nausea), diarrhea or intestinal paresis .
The presence of elevated temperature (up to 38-39 C) in patients with jaundice means the addition of cholangitis . Infection of the biliary tract is considered an unfavorable factor, since the development of purulent complications and liver failure , which aggravates the patient’s condition. It is possible to palpate a tumor only if it is significant in size or if it has metastasized. An objective examination, in addition to jaundice, reveals an enlarged liver and gall bladder.
A companion to jaundice is itching of the skin, which is caused by irritation of skin receptors by bile acids. Most often it appears after jaundice with a high level of bilirubin , but sometimes patients even before the jaundice period complain of itchy skin. It is intense, worsens at night, and significantly worsens your well-being, as it causes insomnia and irritability . Nausea and vomiting occur both with cancer of the head and with tumors of the tail and body and are the result of compression of the duodenum and stomach by the tumor.
Symptoms also include pain in the upper abdomen. In the initial stages, the pain weakens when the patient bends forward, and with a widespread process it becomes painful, quickly causes asthenia in the patient and requires the use of painkillers. If the tumor is located in the head of the gland, the pain is localized in the epigastrium , and with a tumor in the body and tail, it spreads to the left hypochondrium and left lumbar region. When irradiating to the back, which simulates the clinical picture of renal pathology, one may suspect the spread of the process into the retroperitoneal space. Aching, dull pain in the epigastrium is often regarded as “gastritis”, “peptic ulcer”, “cholecysto-pancreatitis”.
Systemic manifestations of pancreatic cancer, regardless of location, include:
- Loss of appetite. Anorexia is observed in more than half of patients with head cancer and in a third of patients with its localization in other parts of the gland.
- Weight loss. Weight loss is the most important symptom. It is associated with decreased appetite, intestinal indigestion due to blocked ducts, and cancer cachexia . Weight loss is considered the most common symptom.
- Increased blood sugar levels. Some patients develop diabetes because insulin is suppressed, causing polydipsia (increased thirst) and polyuria (increased volume of urine produced).
The above symptoms are signs indicating inoperability or questionable operability. Detection of ascites, determination of the tumor by palpation, stenosis of the stomach (its outlet) exclude the possibility of radical removal of the tumor.
A benign tumor is either a serous neoplasm or simple cysts and pseudocysts. Most cysts are asymptomatic. In rare cases, glandular adenoma has striking manifestations in the form of acute pancreatitis and jaundice . Compression of the stomach or duodenum by a large cyst causes nausea, vomiting, jaundice and makes it difficult to empty these organs. The appearance of abdominal pain in most cases indicates degeneration into a malignant tumor (especially with pseudocysts). The pain can also be localized in the back, simulating spinal diseases.
Symptoms of Zollinger-Ellison syndrome include gastrointestinal ulcers About half of patients experience esophagitis. In 75% of patients, ulcers develop in the stomach and in the initial parts of the duodenum. The possibility of their appearance in the jejunum and in the distal parts of the duodenum cannot be excluded. Ulcers can be single or multiple (more often with postbulbar localization).
The clinical manifestations of ulcers are the same as those of a regular peptic ulcer , but a characteristic feature is persistent pain and an unsatisfactory response to antiulcer treatment. Ulcers with this syndrome often recur and are also accompanied by complications: perforation , bleeding and stenosis . Complications are very severe and are the main cause of death.
In addition, duodenal ulcers are combined with diarrhea , esophagitis , steatorrhea , increased calcium levels, accompanied by vomiting and weight loss. A characteristic symptom of this syndrome is diarrhea, which is more common in women. In half of patients, diarrhea is the first manifestation. Hypersecretion of hydrochloric acid damages the jejunal mucosa, which is accompanied by increased motility and slower absorption of water and sodium. At this pH value, pancreatic enzymes (lipase) are inactivated. Fats are not digested, their absorption decreases, steatorrhea and weight loss progresses.
Symptoms and course of pancreatic head cancer
Cancer of the head of the pancreas differs significantly in clinical picture from cancer of the rest of the pancreas. The predominant and even constant symptom of head cancer should be considered persistent severe jaundice and cachexia. Dyspeptic gastrointestinal symptoms, pain, ascites, and palpable swelling are often observed; much less often - glycosuria.
The onset of the disease, as always with cancers of internal organs, is hidden. Sometimes mild dyspeptic symptoms from the stomach or intestines are observed. At first, there is more often a tendency to constipation than to diarrhea, which may come to the fore in the further course of the disease. In some cases, patients complain of heaviness in the stomach or right hypochondrium. However, the sensations of heaviness at first are vague and in no way can be called painful. Quite soon, jaundice appears, noticeable at first only on the connective membrane of the eyes. It then becomes visible on the face, abdomen, torso and limbs. Once it appears, jaundice cannot significantly weaken, much less disappear; on the contrary, it becomes more pronounced day by day. As a result, the skin gets a special dark yellowish-olive color, most pronounced on the face. This skin color on an emaciated patient is so characteristic that it sometimes allows for probable recognition even at a distance.
During a period of severe jaundice, one can usually notice an enlarged liver and a more or less distended gallbladder, in the form of a tense pear-shaped tumor lying directly under the liver. In parallel with the development of jaundice, stool becomes discolored quite quickly. Sometimes fatty stool appears. Along with neutral fat, you can find a large amount of fatty acids and soaps. The presence of the latter chemical formations occurs only in the later stages of the disease, with great destruction of the gland; they cause the acrid, fetid odor of feces. All these intestinal phenomena develop with cancer of the head of the pancreas much less frequently than with chronic inflammation of the gland, which ultimately leads to a strong development of connective tissue and to the death of the active elements of the gland.
With the relatively rapid development of cancer, which also occupies only part of the parenchyma, most of the gland continues to function as an excretory and incretory organ. This last circumstance makes the rare occurrence of glycosuria in cancer of the head of the pancreas completely understandable.
Closure of the bile duct and the congestive jaundice caused by it appear in a relatively early period of the disease, while compression of the portal vein is caused only by a greatly expanded tumor. This leads to the appearance of ascites and an enlarged spleen. Swelling of the lower half of the body due to compression of the inferior vena cava is extremely rare. In general, ascites is a late symptom of the disease and develops after the appearance of jaundice. In debilitated patients, you can sometimes feel a hard, tuberous tumor corresponding to the head of the pancreas.
In advanced cases, metastases are detected in various organs and especially in the liver. Probably, the beginning of cachexia should explain the usually observed lack of free hydrochloric acid in gastric juice. In advanced cases, black stools appear due to the large presence of altered blood. In some cases, this phenomenon depends on the direct transfer of cancer to the duodenum or stomach and bleeding from the resulting ulcer of the mucous membrane. In others, at autopsy, no changes are found in the mucous membrane of the stomach and duodenum.
The course of the disease is quite rapid. Cancer of the head of the pancreas leads to death in a shorter time than cancer of other organs. This, by the way, depends on the fact that pure cancer cachexia is accompanied by exhaustion from the absence of two important digestive fluids in the intestines: bile and pancreatic juice, and in addition, from rapidly increasing changes in the liver parenchyma and the presence of elements in the tissues of the body and in the blood bile. The duration of the disease is considered to be months and relatively rarely extends beyond one year.
Tests and diagnosis of pancreatic cancer
- Ultrasound is the primary examination method.
- Contrast-enhanced computed tomography determines the stage, spread to neighboring organs, metastasis and gives a conclusion about the resectability of the tumor. If the tumor is no more than 2-3 cm in size and no vessels are involved, then it is operable. Computed tomography and magnetic resonance imaging help identify cysts. MRI is used to accurately determine the stages of neuroendocrine tumors. Thus, uneven edges and decreased signal in the venous phase are characteristic signs of poorly differentiated neuroendocrine tumors.
- Diagnosis at an early stage is carried out using an optical spectroscope ( spectroscopy ), which can even detect changes in precancerous formations and allows us to draw a conclusion about the need to remove the cyst. When identifying malignant cysts, the accuracy of spectroscopy reaches 95%. The diagnosis made by spectroscopy coincides with postoperative histological analysis.
- To determine the level of blockage of the bile and pancreatic ducts, retrograde endoscopic cholangiopancreatography . It is carried out using a duodenoscope and a fluoroscopic unit using radiopaque agents ( Triombrast , Ultravist ).
- Multidetector SCT is an informative preoperative method. Allows you to determine the operability of a tumor based on: size, spread to large vessels, relationship with surrounding organs (extend to the hepatoduodenal ligament, mesentery of the small intestine), degree of deformation of the bile ducts.
- Aspiration biopsy confirms the diagnosis, but is recommended only in cases where imaging tests are equivocal. It is preferably performed under ultrasound guidance.
- Determination of tumor markers in the blood. The most sensitive, specific and approved marker for cancer of this organ is CA-19-9. In healthy people, its content does not exceed 37 units, but with this disease it increases tens, hundreds and thousands of times, since it is produced by cancer cells. But in early cancer, the level of CA-19-9 is not increased, so this method cannot be used to conduct screening studies and identify early forms. The addition of two more biomarkers (tenascin C and tissue factor inhibitor) to this marker allows detection of early stages of cancer.
- For neuroendocrine tumors, chromogranin A is used as an immunohistochemical marker, but it has low significance in the diagnosis of this type of tumor. However, high levels of chromogranin A (>156.5 ng/ml) indicate the presence of metastases.
Malignant tumors
This type of tumor is not only difficult to diagnose, but also difficult to treat. We can say that it cannot be cured. You can only extend a person’s life for a certain period. It is very difficult to determine the presence of a tumor, since in the early stages of its formation it does not appear at all. There are also situations when the symptoms of cancer are invisible until stage 4.
Varieties:
- squamous cell carcinoma;
- adenocarcinoma;
- endogenous cancer;
- acinar cell carcinoma;
- cystadenocarcinoma.
Tumor of the head of the pancreas
Due to the fact that the tumor on the head is located in close proximity to the gastrointestinal tract, it first of all makes itself felt by symptoms of digestive disorders. A person experiences nausea and vomiting, diarrhea, excrement becomes discolored, bloating is noted, and the urine darkens. In addition, there are several other symptoms:
- an increase in glucose levels in the bloodstream;
- decreased appetite;
- weight loss;
- obstructive jaundice. This symptom is considered characteristic. Obstructive jaundice occurs when a tumor compresses the bile duct.
The danger of a neoplasm also lies in the fact that it can grow into other organs. This is observed at the 2nd or 3rd stage of its formation. At 4, the spread of metastases to other organs is noted. In this case, surgical intervention is no longer performed. The basis of treatment is supportive therapy.
Diet
Diet for pancreatic cancer
- Efficacy: no data
- Timing: constantly
- Cost of products: 1500-1600 rubles. in Week
In the initial stages of the disease, patients can eat regular food and take pancreatic enzymes. Subsequently, most patients experience anorexia and malabsorption syndrome due to a violation of the exocrine function of the gland. High-fat foods are excluded from the diet of patients. The diet reduces the amount of fiber because it absorbs enzymes, reducing the supply of nutrients. Nutrition for pancreatic cancer should be organized as for any cancer, and it must be taken into account that its insufficiency in such patients only aggravates metabolic disorders.
When the patient's condition is severe or when they are unable to consume enough calories and with progressive weight loss, they resort to oral administration of mixtures intended for enteral nutrition, in small sips (siping) or through a tube. This is a type of therapeutic nutrition in which hypercaloric drinks and creams with increased taste provide cancer patients with reduced appetite with all the necessary substances.
The administration of liquid mixtures can stop weight loss and normalize nutritional status for further antitumor treatment programs. With a smaller volume of liquid, the mixtures have a high calorie content, they are balanced, enriched with vitamins and microelements, and contain omega-3 fatty acids. Currently, mixtures for oral administration have been developed, which are positioned as specifically intended for use in patients with cancer to prevent the development of cancer cachexia . These can be mixtures based on whey protein peptides ( Peptamen ) or a mixture with a high content of protein, omega acids, antioxidants and reduced carbohydrates ( Supportan Drink ).
Can it be cured?
The prognosis depends on the stage of the disease (location of the tumor within the boundaries of the organ or behind it, involvement of neighboring organs and the presence of metastases in them), localization of the tumor in the gland, the state of the body systems and the degree to which the operating room is equipped with the necessary equipment.
If all favorable conditions are present, measures can be taken regarding cancer:
- In stage 0 - radical excision of the tumor with mandatory gamma irradiation following the operation.
- In I - the most radical intervention (either with excision of the entire gland, or limited to its resection, or using the Whipple technique) with radiation therapy.
- At stages II and III, exclusively palliative operations can be performed to eliminate mechanical obstacles created for digestion by the gland itself or a block from it and neighboring organs (to overcome obstruction of the ducts, intestinal obstruction) or measures can be taken to suturing perforations of the stomach and intestines.
- In stage IV, due to the extremely serious condition of the patient, whose body is not able to bear any serious load, and the metastasis of the tumor to distant organs, oncologists are no longer able to offer the patient anything.
Thus, complete healing is possible only at 0 or in the initial stages of stage I.
Video about pancreatic cancer:
Consequences and complications
Complications include:
- Metastases to the lungs, lymph nodes and liver. Peritoneal metastases can compress the intestine and cause constipation or intestinal obstruction .
- The occurrence of thrombosis (with adenocarcinoma the risk is much higher than with squamous cell carcinoma).
- Stenosis and bleeding when the tumor grows into the stomach and duodenum.
- Hepatocerebral insufficiency , which is manifested by lethargy.
- Splenomegaly and bleeding from the veins of the esophagus when the tumor is located in the body or tail.
Forecast
Survival rates for patients with this pathology are very low due to the lack of diagnostic capabilities to detect the disease in its early stages. Despite the treatment, the prognosis for life expectancy for pancreatic cancer remains unfavorable. It all depends on the stage of the disease and the presence of gene mutations. In 80-90% of patients, the tumor turns out to be inoperable at the time of diagnosis (metastasis or invasion of nearby organs), which has a poor prognosis in the future. Survival also depends on the genetic profile. Tumors harboring DAXX or ATRX mutations are associated with poor prognosis. By studying the genetic profile, it is possible to identify in advance patients who need early and aggressive therapy. Expression of the SerpinB2 gene in the body of the gland in adenocarcinoma is not associated with metastasis, therefore such patients have long survival.
Treatment methods are also important in prognosis. After radical surgical treatment, survival rate does not exceed 15%, and the remaining patients die within 5 years after treatment. Therefore, the surgical method is supported by chemotherapy treatment. Combinations of several drugs significantly improve the prognosis.
How long can you live with pancreatic cancer? After surgical treatment, the prognosis remains unfavorable, since the relapse rate is 80-90%. Five-year survival after surgery is achieved by 25-30% of patients without metastases and only 10% of patients with metastases. If combined chemotherapy is administered after surgery, 29% of patients live 5 years. The type of tumor also affects life expectancy.
How long do people live with stage 4 pancreatic cancer? Since this stage is characterized by a metastatic process, the lifespan for stage 4 pancreatic cancer is 3-6 months. How do patients die? Departure from life is individual. Typically, patients develop severe pain that requires the prescription of narcotic drugs; all patients develop cachexia , which leads to protein-energy malnutrition. Protein deficiency reduces immunity, and the enzymatic function of the gland is further impaired. Decreased immunity increases the risk of infections. The presence of cachexia limits the ability to fully administer chemotherapy . Patients spend more time sleeping, and there is detachment, lethargy and apathy. We must try to organize good care for the sick to give them the opportunity to die peacefully.
List of sources
- Veligotsky N.N. Obstructive diseases of the pancreaticoduodenal zone / N.N. Veligotsky, A.N. Veligotsky. – Kharkov: Planeta-Print, 2015. – 136 p.
- Malyarchuk V.I., Klimov A.E., Pautkin Yu.F. Biliopancreatoduodenal cancer: Monograph. – M.: RUDN Publishing House, 2006. – 444 p.
- Galperin E.I. Lectures on hepatopancreatobiliary surgery / E.I. Galperin, T.G. Dyuzheva. – M.: Vidar, 2011. – 536 p.
- Shchepotin I.B., Lukashenko A.V., Kolesnik E.A. et al. (2011) Pancreatic cancer: criteria for resectability. Clinical Oncology, (4(4)): 65-71.
- Patyutko Yu.I., Kotelnikov A.G., Abgaryan M.V. Modern surgical and combined treatment of patients with exocrine cancer of the head of the pancreas and organs of the periampullary zone. Practical oncology. T.5, N2, 2004, pp.94–107.
Tumor Papilla Vateri of the pancreas
This formation can affect both the pancreas and duodenum. The tumor received its name because of its formation in the place where the bile and pancreatic ducts adjoin the duodenum. This border zone is called Papilla Vateri.
In development, the Papilla Vateri tumor is similar to ductal adenocarcinoma, with the only difference being that against the background of this formation, jaundice develops faster. In this case, the disease can be detected earlier than ductal adenocarcinoma.
Prognosis for pancreatic cancer in terms of lifespan depends on the stage of the tumor. It should be borne in mind that any delay in diagnosis and treatment leads to a significant reduction in life expectancy. If at stage 1 life expectancy is calculated in years, then at stage 4 it is calculated in months.