What is Zollinger-Ellison syndrome?
Zollinger-Ellison syndrome is the occurrence of one or more tumors in the head of the pancreas or small intestine.
The disease is rare, affecting one person in a million. Mostly men aged 20-50 years are affected. Tumor growth begins with islet cells of the pancreas. Neoplasms can be either malignant or benign. The essence of the syndrome is that they produce gastrin, a hormone that stimulates the production of hydrochloric acid in the wall of the stomach. Excess acid leads to the appearance of stomach and duodenal ulcers.
Treatment
Persons with Zollinger-Ellison syndrome are treated in the gastroenterology or surgical department of a hospital. If a malignant tumor is present, patients are hospitalized in an oncology clinic.
Patients with gastrinoma must follow a certain regimen and diet. Dietary meals are organized depending on the patient’s condition. The goal of diet therapy is to reduce irritation on the gastrointestinal tract, relieve inflammation, and accelerate the healing of ulcers. You should eat in small portions up to 6 times a day. Food must be steamed, boiled, baked and consumed pureed.
Conservative therapy is aimed at rapid healing of ulcers, reducing the acidity of gastric juice, and preventing relapse. Patients are usually prescribed the following medications: Omeprazole, Ranitidine, Famotidine, Platiphylline, Pirenzepine, Gastrocepin, Octreotide. All these drugs belong to different pharmacological groups, but have a single effect - antiulcer and antiproliferative. Since the risk of recurrence of ulcers is very high, these drugs are prescribed for life in high doses.
Surgical treatment involves removing a potentially malignant tumor. Ideally, the tumor should be completely removed, which will provide the most favorable prognosis. After the operation, the material is sent for histology, which is used to determine the benignity of the tumor. If the formation is located in such a way that it cannot be reached, it is possible to remove part or all of the organ. Patients are advised to have their stomach removed. In this case, the tumor is not removed. Gastrin has no effect on the organ, and symptoms of the disease no longer appear.
longitudinal duodentotomy, removal of gastrinoma
Types of operations:
- Enucleation is the removal of a gastrinoma without cutting its membrane.
- Pancreaticoduodenectomy - removal of part of the pancreas and duodenum.
- Distal pancreatectomy.
- Subtotal resection of the pancreas.
- Selective embolization of gastrinoma.
- Gastric resection.
- Total gastrectomy.
- Laparoscopy is a common procedure that does not require a complete opening of the abdominal cavity, does not leave scars, and reduces the risk of bleeding and complications.
- If there are metastases in the liver, its resection is performed.
After surgery, the patient is prescribed vitamin B12 and special calcium supplements.
Often patients seek medical help when there are already metastases in the internal organs. In such cases, complete cure after surgery can be achieved only in 30% of patients.
Chemotherapy is widely used in the presence of malignancy. It suppresses tumor growth. However, even such treatment does not guarantee a favorable outcome. Patients are prescribed a combination of drugs - “Streptozocin”, “Fluorouracil”, “Doxorubicin”.
Symptoms and signs
The symptoms of the disease are very similar to those of a gastric ulcer. This is a dull, burning pain in the area between the navel and the sternum. It occurs between meals and at night, i.e. when the stomach is empty. The pain lasts from several minutes to several hours, then goes away.
Also, manifestations of Zollinger-Ellison syndrome can be:
- diarrhea
- bloating (flatulence)
- discomfort in the upper abdomen. The patient has the impression that someone is “gnawing” in the pit of his stomach. There may also be a sensation of burning or burning above the navel.
- belching sour
- heartburn.
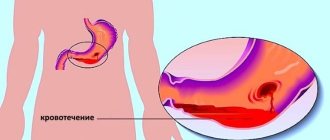
Somewhat less common are bleeding from the upper gastrointestinal tract, unexplained weight loss, and decreased appetite. Sometimes the disease manifests itself only as diarrhea.
Symptoms
The most common clinical sign of the syndrome is the formation of ulcers on the mucous membrane of the stomach and duodenum (in approximately 95% of all cases). Ulcers can be single, or multiple ulcerative lesions can be observed. A distinctive feature of the syndrome is frequent relapses.
Clinical manifestations are in many ways similar to those of gastric and duodenal ulcers. The patient is bothered by pain in the stomach and abdomen, which is constant and is not relieved by medications for the treatment of peptic ulcer.
The pain described by patients is more intense. May be burning or dull. A pattern of pain in relation to eating was also noticed. Weaken after eating. They also have the character of “night pains”. This is due to the activation of the vagus nerve at night.
The patient experiences heartburn and a burning sensation in the chest. And there is also sour belching and bad breath. Upon examination, the tongue is coated with a grayish coating; destruction of tooth enamel and a change in its color to yellow can also be observed.
With reflux syndrome (reflux of gastric contents into the upper parts of the digestive system), pain in the esophagus, tickling and cough may occur.
In many cases, there is heaviness in the stomach, nausea and vomiting. When bleeding occurs, vomit “the color of coffee grounds” is observed.
75% of patients experience chronic diarrhea, which is not entirely characteristic of gastric ulcer. The mechanism of its occurrence is the reflux of hydrochloric acid into the small intestine.
In this regard, the motor function of the small intestine increases, and the absorption of substances decreases. Because of this, a lot of fatty substances are released along with the stool. The stool is copious and watery up to 20 times a day.
Upon examination, the patient’s skin is pale, the tongue is coated with a grayish coating. The mucous membranes are unchanged. When palpating the epigastric region, severe pain is observed. If metastases have spread through the bloodstream to the liver, then you can see its increase in size. In this case, moderate pain in the liver area may be observed.
It should be noted that ulcers on the mucous membrane of the stomach and duodenum have the ability to constantly recur even during antiulcer treatment. This feature causes complications to arise.
Diagnostic methods
To diagnose this rare pathology, it is very important to know your family history. Therefore, a gastroenterologist asks about diseases that are inherited. If one of your relatives has multiple endocrine neoplasia (MEN), the risk is increased. The doctor also finds out the patient’s complaints, clarifies the nature and time of pain, and the presence of other reactions from the gastrointestinal tract. Then the gastroenterologist conducts an examination and palpates (feels) the abdomen.
Blood tests for Zollinger-Ellison syndrome
For accurate diagnosis, the gastrin content in the blood is determined. Elevated levels may indicate a tumor of the pancreas or duodenum. “High” gastrin may be a reaction to antiulcer medications, such as proton pump blockers. Therefore, before taking a blood test, you need to inform your doctor about all chronic diseases and medications you are taking.
In unclear cases, a repeat measurement is carried out after stimulation with secretin: the hormone secretin is administered, then the gastrin level is determined again. With gastrinoma, it grows significantly after stimulation.
Instrumental examination methods
Acidity level measurement. Gastric juice for analysis is taken using a nasogastric tube - a thin rubber tube, which is inserted into the stomach through the nose under anesthesia. High levels of acidity may indicate Zollinger-Ellison syndrome.
Gastroscopy allows you to see ulcers and take a fragment of the bottom of the ulcer for study in the laboratory.
Endoscopic ultrasound: the sensor is installed on the endoscope. The study is carried out directly in the stomach, this increases the chances of detecting tumors.
Somatostatin receptor scintigraphy or octreotide scan. A radioisotope that is safe for the patient is injected into a vein. The substance selectively accumulates in tumor cells, so that they can be observed in a gamma camera. It helps to visualize tumors not only in the pancreas and duodenum, but also in other organs and systems.
CT and MRI are also used to diagnose gastrinoma.
Diagnosis of the disease
For successful treatment of Zollinger-Ellison syndrome, it is extremely important to diagnose it promptly and correctly. Early detection of the pathology is complicated by the similarity of its symptoms to peptic ulcer disease; it is also difficult to detect the localization of tumors due to their often large number and small size. Suspicions of the presence of gastrinoma should arise when traditional treatment of ulcerative defects is ineffective, their atypical location and tendency to relapse.
To diagnose the disease, it is important to study the fasting level of gastrin in the blood serum and in gastric secretions, which is possible when conducting tests with a standardized volume of food or intravenous administration of calcium salts, secretin or glucagon. When using calcium gluconate in patients suffering from Zollinger-Ellison syndrome, the concentration of gastrin increases by more than one and a half times. With intravenous injections of glucagon and secretin, the initial level of the test hormone increases by an average of 70%, and when tested with standardized food it remains unchanged.
Also, when diagnosing pathology, the following is carried out:
- X-ray of the stomach;
- Ultrasonography;
- Ultrasound of the abdominal organs;
- Computed tomography.
The most accurate and at the same time technically complex research methods include selective abdominal angiography, which allows one to determine the level of gastrin in blood taken from the pancreatic veins.
Treatment of Zollinger-Ellison syndrome
Treatment usually begins with medications that reduce the secretion of hydrochloric acid. Then surgery is performed and the gastrinomas are removed.
If the tumors are multiple and cannot be removed surgically, chemotherapy is prescribed.
Medications
The most commonly recommended medications are proton pump inhibitors. These drugs affect the function of the proton pump in cells and reduce the production of hydrochloric acid in the stomach. As a result, the patient notes a decrease in abdominal pain and diarrhea. Use:
- esomeprazole
- lansoprazole
- pantoprazole
- omeprazole
- dexlansoprazole.
If there are contraindications to the prescription of antiulcer drugs, octreotide is used. This substance is similar in its action to the hormone somatostatin; it neutralizes the effect of gastrin.
Chemotherapy is most often administered:
- streptozocin
- 5-fluorouracil
- doxorubicin.