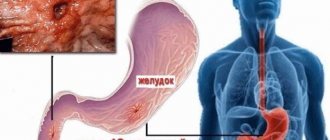
Pathophysiology
The content of the article
Under normal conditions (in a healthy person), the contents of the gastric juice with high acidity periodically enter the esophagus, but internal protective mechanisms either reduce the amount of acid secreted to a minimum or remove the acid, which is quickly removed by “cleansing” the esophagus. Therefore, symptoms of acid irritation of the esophagus are not felt or are minimal.
Mechanisms that protect the esophagus from stomach acid include the lower esophageal sphincter (sphincter) and normal esophageal motility (motility). When these mechanisms are disrupted, reflux occurs and symptoms of GERD occur.
Gastroesophageal reflux
Gastroesophageal reflux without esophagitis. Causes.
Irina, Belgorod
April 18, 2020
Good afternoon
Three weeks ago I began to notice that I was coughing and my voice began to disappear. Deciding that this was my reaction to chlorine, which is now used in large quantities on everything, I went to the therapist, she prescribed an antihistamine - it did not help. I went to an allergist, he diagnosed acute laryngitis of toxic origin and ordered me to avoid contact with bleach, remain silent and consult with an ENT specialist. A week later I went to the ENT specialist - the doctor didn’t find anything. I continued to cough, soften my throat with mineral water inhalations and eucalyptus lozenges. There was no sense in this. To be honest, I was under a lot of stress and couldn’t understand what was going on. I always had a low-grade fever of 36.8-37. At night I started to sweat, my shoulder muscles were very sore. Previously, I had an appointment with a neurologist and he prescribed me mydocalm, however, it did not help me much. And then one fine day I drink tea with sweets and I start to have a strong cough. I’m not a fan of diagnosing myself on Google, but after Googling, I realized that perhaps my cough is from heartburn. I took a Maalox tablet. The cough stopped. After which I decided to see a gastroenterologist, I was diagnosed with gasesophageal reflux without esophagitis. I passed all the tests, all I had to do was do an examination - gastroscopy. I hardly cough, but if I cough, I lose my voice. I am currently prescribed treatment: diet, Nexium, Maalox. I have been taking the medications for 5 days, but there is no improvement. Moreover, if previously I was only bothered by coughing and hoarseness, now I also feel a burning sensation in my chest. I take a walk and it disappears. Over these days I have lost 4 kg (I am fat, with a height of 160 cm I weigh 82.3 kg today), I eat as written in the doctor’s recommendations. I ask respected doctors to answer my questions: 1) how soon can remission occur and how long can it last? It’s not difficult for me to follow a diet, I’m scared for my voice, my ligaments. Is it really true that he suffers from burning and loss of voice all his life? My work does not allow silence. 2) Could taking mydocalm or birth control pills trigger the reflux? 3) Could stress have triggered the reflux? I was very nervous these days, and in general my psychological state leaves much to be desired, I am an anxious person. 4) Why did such a symptom as a burning sensation in the chest appear after taking PPIs and Maalox, previously there was only a cough? 5) Will taking ranitidine help me more than taking a PPI? Thank you in advance for your help. Chronic diseases:
Possibly gastroesophageal reflux without esophagitis
The question is closed
reflux
Etiology: a new approach
The prevailing theory (since 1935) is that GERD occurs when acidic stomach acid spills from the stomach into the esophagus, chemically and mechanically damaging the lining of the esophagus, causing burns, irritation, erosions, and ultimately more serious consequences. However, this traditional theory of chemical and mechanical irritation of the esophageal mucosa cannot fully explain many things associated with the onset, symptoms and course of GERD.
There are now reports that GERD may be an immune-mediated inflammatory disease caused by immune reactions rather than direct chemical damage to the lining of the esophagus by gastric juices. The hypothesis about the etiology of immune GERD is confirmed by one of the clinical studies conducted in the USA. The study results were published in the Journal of the American Medical Association.
Preliminary data from this study showed that T-cell esophagitis, basal cell hyperplasia, and spleen cell hyperplasia were observed in patients with severe GERD treated effectively with proton pump inhibitors (PPIs) after PPI discontinuation, but with resistant superficial cells.
According to study leader at the Dallas Veterans Medical Center, Dr. Kerry Dunbar, This finding suggests that the pathogenesis of reflux disease may be related more to inflammatory mediators and cytokines than to chemical damage to the esophageal mucosa.
The inflammatory immune theory of GEB could more easily and better explain not only the onset and course of the typical symptoms of this disease, but also the pathophysiology of the complications of this pathology - metaplasia of the esophagus and Barrett's mucosa.
Barrett's esophagus
Recent experimental studies in rats also suggest that GERD is more related to immune rather than chemical acid damage to the esophageal mucosa. Reflux and chemical acid irritation are thought to only initiate immune inflammatory responses in the esophageal mucosa and therefore play a less important role.
If the immuno-inflammatory theory of the etiopathogenesis of GERD turns out to be correct, it may be necessary to reconsider the existing regimen for the treatment and prevention of relapses of GERD. It is possible that the location and role of antisecretory drugs (PPIs, H2 blockers) may change.
It is assumed that the immune theory of reflux disease can explain in more detail the causes and essence of not only typical, but also recently described atypical forms (so-called subtypes) of GERD.
Researchers suggest that PPIs and H2 blockers may remain the most important drugs for treating GERD, but treatment regimens for this disease should also include drugs that affect the immune-inflammatory response cascade, especially for more severe and refractory forms of GERD.
Causes
Factors provoking non-erosive gastroesophageal reflux disease, i.e., characterized by reverse flow of contents, are due to the following:
- displacement of the esophageal opening or the upper part of the stomach located at the junction with the esophagus;
- poor diet, obesity or frequent gag reflexes;
- long-term use of medications that weaken the muscles of the valve between the esophagus and stomach.
Smoking and excessive drinking of alcoholic beverages play an important role in the occurrence of GERD. The disease progresses with some skin and vascular diseases caused by impaired blood circulation and inflammation of internal organs.
Treatment of gastroesophageal reflux disease
According to current guidelines, GERD is treated in stages. Goal of treatment: control the symptoms of the disease, treat esophagitis, prevent relapses of esophagitis and complications of the disease.
Treatment of GERD consists of the following steps:
- Lifestyle changes and control of gastric juice secretion (antacids, PSI, H2B).
- If necessary, surgical treatment is used, and corrective antireflux surgery is performed.
Non-pharmacological measures include the following:
- Reducing excess weight;
- Refusal of certain drinks and foods (alcohol, chocolate, citrus fruits, tomatoes), mint, coffee, onions, garlic;
- Frequent meals at regular intervals;
- Sleep at least 3 hours after eating, with your head raised (~ 20 cm);
- Limiting squats, bending, etc.
Eating frequently at regular intervals
Treatment of GERD
Therapy for GERD begins with non-drug methods - dietary and lifestyle changes:
- raise the head end of the bed by 10-15 cm;
- reduce the amount of fat in food, increase the protein content;
- eat small and frequent meals;
- exclude mint, coffee, tea, chocolate (reduce the tone of the esophageal sphincter), spices, citrus juices, alcohol (direct irritant effect);
- do not lie down for two hours after eating;
- do not lift heavy objects (more than 10 kg);
- do not be “bent over” for a long time, including not working in the garden;
- do not do abdominal exercises;
- do not wear tight belts, corsets, tight clothing;
- lose weight;
- stop smoking (nicotine derivatives reduce the tone of the esophageal sphincter).
If possible, after consultation with your doctor, you should stop taking medications that contribute to the occurrence of reflux. Considering that GERD is often combined with other gastrointestinal diseases, dietary table No. 1, 4, is prescribed, depending on the underlying disease. If non-drug methods are ineffective within 2-3 weeks, medications are prescribed:
- Gastroprotectors are the basis of treatment. Helps restore damaged mucous membranes (rebamipide).
- Proton pump inhibitors - reduce the production of hydrochloric acid in the stomach (omeprazole, lansoprazole, rabeprazole).
- H2 blockers, antacids - are prescribed if proton pump inhibitors are not suitable (ranitidine, famotidine, almagel, phosphalugel, gaviscon).
- Prokinetics are drugs that restore normal motility of the gastrointestinal tract (itomed).
When assessing the effectiveness of treatment, you need to keep in mind that ulcers and erosions of the esophagus heal in about eight weeks (for comparison: the healing time for stomach and duodenal ulcers is about 3-4 weeks).
If conservative methods do not help, a surgery called fundoplication is recommended. Part of the stomach is wrapped around the lower part of the esophagus, creating a cuff that prevents the reverse reflux of food.
Antacids
Until the 1980s, antacids were the standard treatment for mild forms of GERD. They are still used to reduce symptoms of mild reflux. Antacids are taken after each meal and before bed.
Taking antacids before bed
Antacids are also useful for side effects: they relieve constipation (aluminum antacids: ALternaGEL, Amphojel), they can increase loose stools (magnesium antacids: Phillips Milk of Magnesia). Aluminum hydroxide increases the pH of the stomach contents to >4 and inhibits the proteolytic activity of pepsin, reducing the symptoms of indigestion. Antacids do not reduce the frequency of reflux, but they do reduce the acidity of the fluid.
Magnesium hydroxide suppresses the symptoms of acidosis and improves digestion. Magnesium hydroxide antacids osmotically retain fluids in the intestine, which distends the intestinal wall, stimulates intestinal motility, and softens stools (laxative effect). When interacting with hydrochloric acid of gastric juice, magnesium hydroxide is converted into magnesium chloride.
New antacids and antirefluxants
Alginic acid salts have been used clinically to relieve symptoms of heartburn and esophagitis for over 30 years. Alginic acid salts have a unique mechanism of action: when interacting with gastric acid, alginates precipitate and form a gel that covers the esophageal mucosa with a protective layer and promotes its restoration.
In vitro and in vivo studies have shown that alginates combine carbon dioxide and some antacid components. Recent kinetic studies have shown that alginates bypass acidic contents and reach the esophagus before the esophageal contents, protecting the organ mucosa from mechanical and chemical irritation from hydrochloric acid. According to clinical studies, alginates also act as a physical barrier, thereby more effectively suppressing reflux.
Alginate products contain antacids, which are acid neutralizing agents that reduce heartburn, but studies have not shown that the effectiveness of these combination drugs depends on their neutralizing properties.
The clinical effectiveness of alginate preparations depends on many factors: the amount and penetration of carbon dioxide released, the characteristics of the molecule, additional ingredients (aluminum, calcium) that have a positive potentiating effect.
Alginate preparations remain in the stomach for several hours, so they last significantly longer and are more effective in suppressing the symptoms of GERD than traditional antacids, they begin to work quickly and last a long time. Alginate preparations are completely safe and are therefore used to reduce the symptoms of reflux in infants, children and pregnant women.
For example, one of these magnesium alginate preparations, Refluxaid, is used in European countries to reduce the symptoms of reflux and acidosis in GERD, peptic ulcers, esophagitis, functional dyspepsia, and other functional and inflammatory diseases of the gastrointestinal tract, manifested by heartburn, reflux, and epigastric discomfort.
Refluxaid drug
The magnesium alginate in Rexluxaid is a natural substance extracted from seaweed. The drug has a high viscosity, which increases anti-reflux effectiveness and duration of action. It has emulsion and swelling properties.
Studies have shown that the highly viscous compound Refluxaid, when ingested into the stomach, creates a physical barrier that binds and neutralizes gastric juice, thereby protecting the esophagus from symptoms of reflux: heartburn, burning behind the sternum, chest pain, epigastric discomfort, etc. Taking these The medication reduces heartburn, acid regurgitation, dysphagia and odynophagia (difficulty swallowing and pain) are reduced, and extrazophaginic symptoms of GERD are also suppressed - cough, hoarseness.
Refluxaid is a prescription medication. It is used for episodic relief of symptoms of acidosis, reflux and esophagitis, on demand or in combination with anti-reflux medications (antisecretory PPIs, H2 blockers, prokinetics).
It has been found that when a person sleeps, magnesium alginate can remain in the stomach for up to 8 hours without breaking down—enough time for the patient to get a good night's sleep. Taking reflux before bed may improve the quality of sleep in a patient with GERD because the symptoms caused by nocturnal reflux will be suppressed.
Treatment methods
First of all, drugs are prescribed to eliminate concomitant symptoms. This happens in order to reduce the risk of developing severe complications and to prevent recurrences of the disease in the form of exacerbation.
The doctor’s first recommendation always relates to changing your usual lifestyle: this implies a complete abandonment of bad habits, limiting the list of medications taken, a diet (repeated, strictly dosed meals) and the obligatory condition of getting rid of extra pounds. It is necessary to exclude any meals three hours before bedtime. Late-night snacking is under no circumstances allowed. The ban includes fried, salty, fatty foods, coffee, tomatoes, citrus fruits, chocolate and soda. Sleep in a special position with the upper body elevated. A complete ban on wearing tight or tight synthetic clothing.
You can’t do without medication. The drugs are designed to protect the integrity of the mucous tissues of the esophagus and stomach, to protect them from the effects of reflux from the stomach. The main group of drugs belongs to antisecretory drugs. These medications are designed to reduce the production of acid and stomach acid at night and when not eating. Proton pump inhibitors are prescribed to patients for the same purpose, to reduce the formation of acids and improve the production of gastric secretions and juices. They balance the level of acidity in the stomach. The most relevant today are drugs with combined effects. These drugs act for quite a long time and are effective.
Despite the absence of damaged areas of the esophagus, unlike the damage caused by gastroesophageal reflux esophagitis disease, it is difficult to treat such a disease; for a long time it is not possible to eliminate the symptoms and develop positive dynamics to improve the patient’s well-being. When making such a diagnosis, it is possible to detect a developing complication - reflux esophagitis.
Antisecretory drugs, H2 receptor blockers
This is the first-line treatment for mild to moderate GERD and grade I-II esophagitis. Four H2 blockers are commonly used in clinical practice: ranitidine, famotidine, cimetidine, and nizatidine. They are more effective in suppressing unstimulated secretion of gastric juice with food and are therefore recommended on an empty stomach or at night.
H2 blockers are effective in the treatment of mild esophagitis (70-80% of patients recover), as well as in antirecessive treatment and prevention of relapses. The effectiveness of H2 blockers decreases with long-term use, leading to tachyphylaxis. An H2 blocker is recommended for patients suffering from nocturnal reflux symptoms, especially in Barrett's temple.
Proton pump inhibitors (PPIs)
These are powerful drugs that suppress gastric secretion. Clinical studies have shown that they are most effective in treating GERD. PPIs are generally well tolerated and cause relatively few side effects. However, PPIs can disrupt calcium homeostasis, exacerbating existing cardiac conduction abnormalities. PPIs increase the risk of hip fractures in postmenopausal women.
Multiple clinical trials have concluded that PPIs are more effective than H2 blockers in controlling GERD symptoms over 4 weeks. And are more effective in treating esophagitis within 8 weeks. It also reports that no one PSI drug was found to be more effective than others in controlling GERD symptoms over 8 weeks.
Although PPIs are the most effective antisecretory drugs, their use, especially over a long period of time, is associated with many side effects. Firstly, PPIs have restrictions on their use: they cannot be used in children under 1 year of age, pregnant or lactating women. PPI use during pregnancy has been shown to increase the risk of birth defects (heart defects).
Restrictions on the use of PPIs
Research conducted in the United States shows that overuse of PPIs has dangerous consequences. Therefore, the US FDA warns doctors and patients that there should be no more than three 14-day courses of treatment per year. Long-term or frequent use of PPIs is associated with an increased risk of bone fractures, hypovitaminosis B12, electrolyte imbalances (primarily hypomagnesemia), muscle spasms, and even seizures.
Excessive suppression of gastric acid secretion when taking PPIs can cause epigastric discomfort, indigestion, increased intestinal infections (C. difficile, etc.), and the risk of aspiration pneumonia. The risk of infectious complications is even higher when PPIs are used with H2 blockers.
Prokinetics
Prokinetics are only effective in treating mild forms of GERD. If GERD is more severe, in addition to prokinetics, drugs that inhibit the secretion of gastric juice are usually prescribed.
Of the prokinetic agents, metoclopramide (10 mg/day orally) is prescribed in European clinics - this is the most commonly prescribed regimen in adults with GERD. Long-term treatment with prokinetic drugs can be dangerous, with serious, even fatal, complications.
ONLINE REGISTRATION at the DIANA clinic
You can sign up by calling the toll-free phone number 8-800-707-15-60 or filling out the contact form. In this case, we will contact you ourselves.
If you find an error, please select a piece of text and press Ctrl+Enter