Sludge in the gallbladder refers to a pathological process that is characterized by stagnation of bile and the formation of a suspension of cholesterol crystals, calcified salts and protein. This syndrome is detected using ultrasound diagnostics. Biliary sludge in the gallbladder refers to the initial stage of gallstone disease.
Sludge gallbladder syndrome
Symptoms of the disease
Biliary sludge - few people know what it is. But this anomaly occurs quite often, as it is characterized by the accumulation of sand in the bile. If the disease is left untreated for a long time, it develops into a more serious pathology called cholelithiasis.
Suspensions in bile are quite difficult to immediately recognize. The patient may not experience any discomfort for a long time. Doctors say that sand appears due to other pathological processes in the body. The trigger mechanism is the primary disease, and after that, disorders in the gallbladder appear.
Gallbladder sludge is characterized by a tingling or numb feeling in the right abdominal area under the ribs. The patient also complains of nausea and discomfort in the gastrointestinal tract. When bending over and eating fatty foods, painful sensations occur and appetite is lost.
In the future, as the pathology develops, the patient may complain of heartburn, belching, and vomiting. There is stool disorder in the form of diarrhea or constipation.
Symptoms of the disease
Sludge syndrome is considered one of those types of diseases when the course of the disease in adults and children is not accompanied by obvious symptoms.
Signs of the disease may be mixed with general symptoms of diseases characteristic of cholecystitis and cholelithiasis. The reason for contacting a specialist may be the absence of a history of such diseases. General manifestations of sediment formation are:
- Quite strong pain in the area of the extreme rib on the right (the pain can be acute or aching);
- Intoxication (weakness, headache, fever);
- Jaundice (its appearance is facilitated by poor outflow of bile secretions);
- Flatulence (if inflammation has spread to the pancreas);
- Heartburn, vomiting, bowel dysfunction.
If any of these symptoms are present, an ultrasound is prescribed and the causes of sedimentation are determined (usually biliary sludge is considered as a basis for the development of other diseases).
Symptoms and causes:
- Pain syndrome is likely at the beginning of the formation of cholecystitis or during the movement of suspensions into the gallbladder, but the presence of the sediment itself does not cause pain;
- Intoxication occurs with pancreatitis and cholecystitis and is considered the main symptom of the inflammatory process;
- Jaundice is caused by a spasm of the duct caused by pain or a stone that has closed the duct, in a word, when the flow of bile is disrupted;
- Flatulence occurs when inflammation of the pancreas begins;
- Dyspepsia syndrome (vomiting, nausea, heartburn, diarrhea) appears when there is a lack of bile entering the duodenum, and digestion fails.
Causes of the pathological process
Flakes in the gallbladder can occur for various reasons. Basically, this disease manifests itself when the pathways in the gallbladder are narrowed due to chronic inflammatory processes.
It can also be caused by obesity due to poor diet and abuse of fatty, fried or salty foods. This phenomenon leads to disruption of the motor function of the gallbladder and intestines.
Sludge in the gallbladder can develop due to surgical interventions on the stomach and feeding through a tube.
One of the decisive factors is leading an unhealthy lifestyle. These include frequent consumption of alcohol, sedentary work and a sedentary lifestyle, and smoking.
Other diseases such as hydrocele of the gallbladder, diabetes mellitus, anemia, cirrhosis of the liver, pancreatitis or cholestasis can also lead to biliary sludge.
Long-term use of antibiotics and uncontrolled use of other medications leads to sedimentation.
Diagnosis of pathology
This phenomenon practically does not manifest itself in any way at the initial stages. Therefore, it is difficult to find out about its existence. When sediment in the gallbladder fills a larger volume than bile, the first symptoms begin to appear. This signals that you need to urgently seek help from a doctor. First of all, the doctor listens to the patient’s complaints and palpates the abdominal area. If pain or unpleasant symptoms occur, the specialist will prescribe an examination.
It includes donating urine and blood to determine the inflammatory process. Using these methods, it is possible to recognize the cause of the disease.
We recommend reading:
Hypotension of the gallbladder
When donating blood for a biochemical analysis, the doctor will be able to identify changes in enzymes in the liver, determine the amount of protein and bilirubin.
To establish an accurate diagnosis, ultrasound diagnostics is performed. When performing this method, it is possible to discern clots and flakes in the gallbladder. The condition of the walls of the gallbladder and nearby organs is also assessed.
After this, duodenal intubation and bile examination are performed.
Using computed tomography and magnetic tomography, it is possible to determine the size of the liver and gallbladder and their changes.
On the frequency of detection of “bile sludge” using ultrasound
Ultrasound scanner HS50
Affordable efficiency.
A versatile ultrasound scanner with compact design and innovative capabilities.
Introduction
With the development of various imaging methods, in particular ultrasonography, specific nosological forms have appeared, among which “bile sludge” (previously not diagnosed using x-ray examination) is found. “Bile sludge” is a mixture of mucus, calcium bilirubinate and cholesterol crystals. It appears when bile becomes thick and viscous, replacing normal bile [1, 2].
There are different points of view regarding the etiology and pathogenesis of sludge. Some view “bile sludge” as a precursor to gallstones, while others view it as a transient, reversible condition of bile balance. “Bile sludge” appears when the ratio of the main components of bile changes or a violation of gallbladder emptying develops.
Considering the etiology of “bile sludge”, it can be classified into secondary and primary. Secondary sludge appears when there is a well-known etiopathogenetic condition: after shock wave lithotripsy for gallstones, gallstone disease, pregnancy [3, 4], liver cirrhosis, obstructive jaundice, hydrocele of the gallbladder, long-term parenteral nutrition [5, 6], diabetes mellitus, sickle cell anemia [7], after taking ceftriaxone [8, 9]. Primary sludge is regarded in cases where none of the above conditions can be identified.
Materials and methods
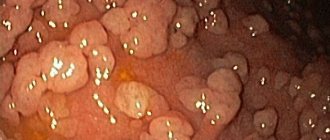
In a study conducted in the USA, “bile sludge” appeared as a hyperechoic formation in the gallbladder with a horizontal level without a posterior shadow, the shape of which slowly changed with the movement of the patient [10]. A characteristic sign of “bile sludge” is a change in its appearance on the scanogram depending on the change in the position of the patient’s body and the slow achievement of a new horizontal level. The general rule is the absence of a distal acoustic shadow. The echogenicity of sludge can vary. Sometimes sludge fills the entire gallbladder, making it difficult to differentiate between liver tissue and the gallbladder. This situation is called “hepatization of the gallbladder” (Fig. 1).
Rice. 1.
Hepatization of the gallbladder, completely filled with sludge.
In addition to the typical appearance, “bile sludge” can have a special appearance, similar to a round polypoidal space-occupying formation with sharp edges or an uneven contour (“tumor-like bile sludge” or “sludge balls” [12, 13]). When the patient's position changes, sludge balls are seen rolling or collapsing, then again forming the original space-occupying formation (Fig. 2-8).
Rice. 2.
Gallbladder half filled with sludge.
Rice. 3.
Large gallbladder with sludge.
Rice. 4.
“Bile sludge” in a patient with liver cirrhosis.
Rice. 5.
Gallbladder filled with sludge in a patient with cirrhosis.
Rice. 6.
Gallbladder and bile sludge.
Rice. 7.
“Bile sludge” in the form of a ball.
Rice. 8.
Ball-like "bile sludge".
Using the definition of “bile sludge,” we prospectively screened 11,800 patients for sludge detection using an ultrasound scanner with 3.5 and 5 MHz convex and sector probes. Ultrasound examination was performed after at least a 10-hour fasting period.
Based on clinical or paraclinical data, we divided sludge into primary and secondary.
results
“Bile sludge” was diagnosed in 68 (0.6%) patients, including 39 men and 29 women. The average age of those examined was 55.3 years. Considering the etiology of sludge, we found secondary “bilious sludge” in 75% of cases (51 patients), and primary in 25% (17 patients) (Fig. 9).
Rice. 9.
Etiology of “bile sludge”.
Secondary sludge was more often found in liver cirrhosis (22 cases), then with concomitant gallstones (15 people) and obstructive jaundice (11 patients) (Fig. 10).
Rice. 10.
Cases of secondary sludge.
Discussion
The presence of “bilious sludge” in 0.6% of patients who underwent ultrasound examination means that this nosological form is relatively rare. While the question regarding secondary sludge is quite clear, the clinical significance of primary “bilious sludge” is not yet fully understood. In a study of 96 patients with gallstones, ultrasound follow-up was carried out for an average of 38 months, and W. Middleton [14] showed that 14 (14.5%) patients developed gallstones, 6 (6.2%) patients with sludge complained of hepatic colic (in the absence of cholelithiasis).
Given that gallstones may develop in a proportion (15%) of patients with primary bile sludge, treatment with ursodeoxycholic acid may be effective [15], but the treatment strategy is not yet well established. Another option is to monitor these patients for a long time and then treat only those who develop small gallstones.
As for tumor-like bile sludge, its ultrasound diagnosis can be difficult because differential diagnosis with cancer and gall bladder stones is required (in particular, bilirubin stones sometimes have a subtle acoustic shadow).
Another aspect that needs to be discussed is the false appearance of sludge when the sound power is mismatched (too much gain). To correctly determine the localization of sludge, it is necessary to monitor its movement by changing the position of the patient’s body. But for a sufficiently experienced ultrasound technician, correctly diagnosing sludge is almost never difficult.
conclusions
With the advent of new imaging techniques, the detection of “bile sludge” has become a reality, which has clinical significance. Its frequency is not so high (0.6% of all cases examined with ultrasound), but individual patients with primary “bile sludge” require follow-up to subsequently decide on possible treatment.
Literature
- Goldberg V. Textbook of abdominal ultrasound. Baltimore: Williams and Wilkins, 1993.
- Terada T, Nakanuma Y, Sat to K, Kono N. Biliary sludge and microcalculi in intrahepatic bileduct. Morphological and X-ray microanalytical observations in 18 among 1,179 consecutively autopsied livers. Acta Pathol JPN 1990; 40(12): 894-901.
- Caruso MG, Giangrande M, Clemente C, et al. Serum lipids and biliary sludge during pregnancy. Minerva Gastroenterol Dietol 1993; 39(2): 67-70.
- Maringhini A, Ciambra M, Baccelliere P, et al. Biliary sludge and gallstones in pregnancy: incidence, risk factors and natural history. Ann Intern Med 1993; 119(2): 116-120.
- Murray FE, Stinchcombe SJ, Hawkey CJ. Development of biliary sludge in patients on intensive care unit: results of prospective ultrasonographic study. Gut 1992; 33(8): 1123-1125.
- Sitzmann JV, Pitt HA, Steinborn PA, et al. Cholecystokinin prevents parenteral nutrition induced biliary sludge in humans. Surg Gynecol Obstet 1990;170(l):25-31.
- Nzeh DA, Adedoyin MA. Sonographic pattern of gallbladder disease in children with sickle cell anemia. Pediatr Radiol 1989; 19(5): 290-292.
- Michielsen PP, Fiersens H, Van-Maercke YM. Drug induced gallbladder disease. Incidence, aetiology and management. Drug Saf 1992; 7(1): 32-45.
- Shiffman ML, Keith FB, Moore EV. Pathogenesis of ceftriaxone-associated biliary sludge. In vitro studies of calcium-ceftriaxone binding and solubility. Gastroenterology 1990; 99(6): 1172-1178.
- Angelico M, De-Santis A, Capocaccia L. Biliary sludge: a critical update. J Clin Gastroenterol 1990; 12(6): 656-662.
- Fakhry J. Sonography of tumefactive biliary sludge. Am J Roentgenol 1982; 139:717.
- Cann R. Gallbladder and biliary tree. In: Kawamura DM, eds. Diagnostic medical sonography - a guide to clinical practice. Philadelphia: Lippincott Co., 1992.
- Hisami A. Ultrasonic characteristics of tumefactive biliary sludge. J Clin Ultrasound 1986; 14: 289-292.
- Middleton W. Gallbladder. In: Textbook of abdominal ultrasound. Baltimore: Williams and Wilkins, 1993.
- Guma C, Violaq L, Apestegui C, et al. Therapeutic efficacy of ursodeoxycholic acid in persistent gallbladder lithiasis and persistent biliary sludge: preliminary results of a multicenter experience. Acta Gastroenterol Latinoam 1994; 24(4): 233-237.
Ultrasound scanner HS50
Affordable efficiency.
A versatile ultrasound scanner with compact design and innovative capabilities.
Treatment process
How and with what to treat this pathology? During diagnosis, the condition of the gallbladder and the ability to perform functions are determined. The treatment process depends on what type of biliary sludge is observed.
Drug therapy
If gallbladder sludge syndrome has moderate symptoms, then treatment is not required. In this situation, all efforts are directed towards identifying and eliminating the root cause. It is imperative to follow a specialized diet.
The second group of sludge syndrome involves conservative treatment. The problem can be eliminated with the help of medications without resorting to surgery.
Treatment of biliary sludge involves the use of drugs that include ursodeoxycholic acid and bile acids. Their action is aimed at protecting liver cells and eliminating harmful substances from the body. Such remedies include Ursosan, Cholenzym, Ursofalk, Allochol, Holosas.
If the patient periodically experiences painful sensations in the right region, then antispasmodic drugs are prescribed in the form of No-shpa, Drotaverine or Spasmalgon.
If an inflammatory process is detected, antibacterial agents are prescribed.
As an additional method of treatment, you can resort to traditional methods. The simplest recipe is to drink water with soda on an empty stomach after sleep. It is generally accepted that soda is an alkaline substance that can dissolve cholesterol and calcified stones.
If there is no effect from drug therapy, the patient is prescribed surgery to remove the gallbladder.
We recommend reading:
Parasites in the gallbladder
Treatment
The tactics to combat the disease depend both on the severity of the clinical signs and on the results of the diagnostic studies performed. Both traditional drug therapy and folk remedies are used. Diet also plays an important role in getting rid of pathology. However, for effective treatment of sludge syndrome, you need to see a doctor. Otherwise, there is a high risk of complications.
Drugs
Therapy is aimed at removing clots from the gallbladder. Symptomatic treatment is also prescribed. The following drugs are used for this:
- Products based on ursodeoxycholic acid are among the most effective. Examples of such medications are Ursosan and Ursofalk. These drugs are taken in a course and help remove sludge from the gallbladder.
- To improve the effect of the use of ursodeoxycholic acid, antispasmodics such as No-spa and Papaverine are prescribed. They contribute to the expansion of the excretory duct and alleviate the course of the disease.
- When inflammatory processes are detected, the prescription of antibacterial therapy is justified. Broad-spectrum drugs are used, for example, penicillins and cefazolins.
Traditional methods
It is also possible to alleviate the condition of patients at home. Before using prescriptions, it is recommended to consult your doctor:
- St. John's wort has a pronounced anti-inflammatory effect and also promotes the flow of bile. You will need a tablespoon of dried herb, which is poured with a glass of boiling water and simmered on fire for 15–20 minutes. The broth is filtered, cooled and drunk 50 ml three times a day before meals.
- Dill is widely used in the treatment of gastrointestinal pathologies. You will need 2 tablespoons of plant seeds. They are poured with 400 ml of water and boiled for 15 minutes. Cool the finished product and drink half a glass 3-4 times a day before meals.
Adverse consequences
Don't let the disease get worse. The treatment process must be completed. Without adequate treatment, sediment in the gallbladder turns into stones, which can become stuck in the ducts. This process will lead to the development of cholecystitis.
Other complications may occur in the form of acute pancreatitis, biliary colic, cholestasis, and acute cholangitis.
If the stones reach large sizes, they damage the walls of the organ or get stuck in the bile ducts. Then this phenomenon leads to rupture of the gallbladder.
Symptoms
The clinical picture of the pathology is often blurred and resembles that of chronic inflammation of the gallbladder, especially in its initial stages. Cholesterol crystallization accelerates the process of bile thickening, which is clinically manifested by more pronounced symptoms. When there is more thick sediment in the bladder than normal bile, the condition of patients worsens sharply and the risk of stone formation increases significantly.
The main manifestations of the pathology can be combined into the following syndromes:
- The pain syndrome is manifested by heaviness, discomfort and unpleasant sensations in the hypochondrium on the right. The pain has a pulling, tingling or pressing character and often intensifies to biliary colic, radiating to the lower back, shoulder girdle, under the shoulder blade, and neck. Persistent abdominal syndrome occurs spontaneously or worsens over a long period of time.
- Intoxication syndrome. Stagnation of bile is a common cause of general intoxication, manifested by fever, fatigue, cephalalgia, and drowsiness.
- Jaundice. Yellowing of the skin and mucous membranes is associated with a violation of the outflow of bile due to a stone blocking the duct or its severe spasm. The stool in patients becomes discolored and contains a lot of fat, and the urine darkens.
- Dyspeptic syndrome is manifested by bitterness in the mouth, sudden loss of appetite, belching, heartburn, nausea and vomiting after eating, constipation or diarrhea, flatulence and rumbling in the stomach. Similar signs appear when little bile enters the duodenum.