Anatomy of the vagus nerve
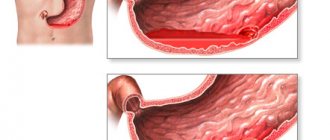
The vagus nerve (nervus vagus) is the largest cranial nerve in our body; it innervates almost all organs of our body, regulating their function. Like other cranial nerves, the vagus nerve is paired; there is a left and a right vagus nerve. Coming out of the cranial cavity, it gives numerous branches to the structures of the head, neck, larynx, lungs, and heart. Going down the esophagus, plexuses of fibers form vagus trunks. The right vagus trunk is located along the posterior surface of the esophagus, and the left vagus trunk passes into the abdominal cavity along the anterior wall of the esophagus.
vagus nerve diagram
After passing through the diaphragm, the abdominal and hepatic branches depart from the vagus trunks; the anterior and posterior nerves of Latarget pass along the lesser curvature, from which branches extend to the upper and middle thirds of the stomach. The terminal part of the Latarget nerves branches in the region of the pylorus in the form of a “crow’s foot”.
The main function of the vagus nerve for the gastrointestinal tract is to stimulate secretion and enhance peristalsis. Its branches branch in the gastric mucosa and innervate glandular cells. With increased tone of the vagus nerve, the secretion of hydrochloric acid increases. And increased acidity is the main pathogenetic mechanism that contributes to the development of ulcerative and erosive lesions of the duodenum (to a lesser extent, the stomach).
Therefore, the idea of surgical denervation of the gastric glands has found application in practice and gives quite good results. With the emergence of new drugs that suppress secretion (proton pump inhibitors), the indications for vagotomy have narrowed significantly.
It should be noted that acid-forming cells are located mainly in the area of the fundus of the stomach and its middle third, therefore the most successful option for vagotomy is the selective intersection of the branches innervating these sections while preserving the remaining nerves.
Vagotomy | Diagnostics and treatment in Israel
Vagotomy is an operation that involves cutting the main trunk or branch of the vagus nerve. This nerve, which is the X pair of cranial nerves, contains sensory and motor nerve fibers. The vagus nerve branches into two trunks: left and right.
The left vagus nerve runs along the anterior surface of the esophagus, and the right one along the back. The vagus nerve enters the abdominal cavity through the esophageal or aortic opening in the diaphragm. These nerve trunks give branches to the liver, stomach and other internal organs.
Descending to the stomach, the right and left branches of the vagus nerve give rise to many branches that spread over its surface and are called Laterger branches.
In the treatment of gastric and duodenal ulcers, this type of surgery has been used since the beginning of the 20th century. The positive effect on the course of the disease is due to a decrease in stimulation of the parietal cells of the stomach.
Normally, these cells produce hydrochloric acid, which is necessary for digestion in the stomach. However, with a peptic ulcer, the production of this substance becomes excessive, which provokes the progression of the ulcer.
After crossing the vagus nerve and its branches, this pathological factor is eliminated and a favorable environment is created for the healing of the ulcerative defect.
In some conditions, vagotomy is not indicated or even contraindicated:
- Extremely high levels of acid-producing function of the stomach (in this case, vatomy may simply be ineffective)
- Disorders of the motor-evacuation function of the stomach
- Peritonitis
- Infectious diseases
- Bleeding in the abdominal cavity
- Decompensated stage of cardiopulmonary diseases
- Severe coagulopathies
- Malignant neoplasms
Preoperative preparation for vagotomy involves a thorough examination of patients:
- Esophagogastroduodenoscopy is necessary in the diagnosis of peptic ulcer disease to assess the condition of the gastric and duodenal mucosa, examine the ulcerative defect of the organ wall, and monitor the dynamics of treatment.
Gastroduodenal intubation allows you to assess the condition of the secretory apparatus of the stomach and duodenum. Fractional intubation is carried out with sampling of gastrointestinal juice on an empty stomach, after a test breakfast, and stimulation of secretion. - X-ray examination of the stomach - helps in identifying ulcerative defects, assessing the motor-evacuation function of the stomach and duodenum.
Several surgical techniques have been developed:
- Truncal vagotomy - the scope of the operation consists of the intersection of both vagus nerves. In this version of the operation, the nerve trunks are isolated at the level of the esophagus
- Selective vagotomy - with this type of operation, the branches of the vagus nerve are intersected after the celiac trunk departs.
This method of vagotomy allows one to preserve the influence of the vagus on the innervation of the small intestine, while inhibiting gastric secretion. - Selective proximal vagotomy or highly selective vagotomy is performed with preservation of the Laterger branches, hepatic and celiac branches of the vagus nerve.
Vagal denervation of only the upper two-thirds of the stomach is observed, which makes it possible to achieve the desired effect with a small number of complications.
The classic operation is performed using general anesthesia and making a midline incision from the xiphoid process of the sternum to the umbilical region.
The postoperative period lasts 10-14 days.
In Israel, laparoscopic vagotomy is more often used. This operation does not require such a wide abdominal incision. Surgical intervention is performed through small punctures in the abdominal wall 2-3 mm long. Through 3-4 such holes, video lighting equipment is inserted into the abdominal cavity, to which a video camera is connected, transmitting the image to the monitor screen.
Sterile carbon dioxide is injected into the abdominal cavity to create a working space as the anterior abdominal wall is lifted above the internal organs. Thus, the surgeon manipulates the abdominal cavity using endoscopic instruments and sees his actions on the monitor. The branches of the vagus nerves are identified and their intersection is performed at the required level.
In addition to the classic intersection of nerve trunks, electrocoagulation and chemical vagotomy are also used. In the first option, a section of the vagus nerve is exposed to an electrocoagulator, which disrupts the integrity of the nerve fibers.
During chemical vagotomy, a special solution based on novocaine and ethanol is injected into the area of the lesser curvature of the stomach.
As a result of degenerative processes in the area of influence of the drug, the stimulating effect of the vagus nerve on the stomach cells in this area ceases.
Types of vagotomy
According to the level of denervation:
- Truncal vagotomy. This procedure destroys the vagus trunks, and not only the stomach, but also the liver, gallbladder, small and large intestine are deprived of innervation. In this case, the drainage function of the stomach is disrupted (due to weakened peristalsis, food stagnates in the stomach cavity). Such vagotomy should always be combined with drainage operations (most often pyloroplasty or gastroduodenostomy).
- Selective vagotomy. In this type, the anterior and posterior nerves of Laterger are separated below the origin of the abdominal and hepatic branches. In this case, the innervation of the intestines and liver is not affected, but the function of the pylorus is impaired. Such vagotomy also requires drainage surgery. Currently, it is used very rarely, since it does not have any special advantages over the stem one, and technically it is much more difficult to carry out, especially in emergency situations.
- Highly selective vagotomy (selective proximal vagotomy). This is denervation of only the fundus and body of the stomach (sections containing acid-producing cells) while maintaining the innervation of the pylorus. Another name for this type of surgery is parietal cell vagotomy [PCV]. This type of vagotomy has the best results and does not require drainage operations. However, it is also the most technically complex and is not always acceptable in case of emergency complications.
By access:
- Open vagotomy.
- Laparoscopic vagotomy.
Vagotomy in combination with other operations:
- With suturing of a perforated ulcer.
- With gastric resection. The combination of vagotomy with resection allows to reduce the number of postoperative ulcers of the anastomosis, as well as reduce the volume of resection. Many centers now use hemigastrectomy in combination with vagotomy instead of classical resection of 2/3 of the stomach.
- With pyloroplasty. This is a procedure for expanding the outlet of the stomach; it most often accompanies trunk and selective vagotomy.
- With drainage operations (gastroduodenostomy, gastrojejunostomy).
- With fundoplication.
Vagotomy of the stomach: types, surgical technique, proximal, stem, selective, reviews
Surgical intervention in the treatment of gastric and duodenal ulcers includes vagotomy. The procedure involves excision of the vagus nerve (main trunk or branch), which reduces the secretion of hydrochloric acid into the stomach. This promotes healing, decreased acidity and successful healing of ulcers.
What is the operation?
The discovery of this method belongs to several scientists (Brody, Exner, Bircher), who since 1814 have proven a positive effect in the treatment of ulcers of the gastric mucosa.
The practical use of vagotomy occurred in 1943 by the American surgeon Lester Dragster. After this, the method was improved and made it possible to identify several types of vagotomy.
With the development of the pharmaceutical industry and the advent of new types of drugs that regulate the production of hydrochloric acid, vagotomy has lost its popularity. In 1993, a Yale University conference decided to abolish this type of surgery as a treatment option for ulcers.
Types of gastric vagotomy
The use of various surgical techniques has made it possible to increase the effectiveness of treatment for various groups of patients.
Classification is carried out according to the following criteria:
- According to the level of denervation: complete or partial excision of the nerve fibers responsible for the production of hydrochloric acid in the stomach.
- By access: abdominal (open) and laparoscopic.
- Vagotomy in combination with other operations gives better results. Most often used with suturing of perforated ulcerated areas or drainage procedures.
The completeness of the operation (success) is determined by a decrease in the acidity level. Typically, tests and pH measurements of gastric contents are used to determine this indicator. If the acidity level is within 5, the surgical intervention is considered successful.
Indications
Despite the relatively infrequent use of this method in modern medicine, for medical reasons it may be necessary to perform vagotomy in certain groups of patients.
Basically, this operation is performed in the following cases:
- In the absence of effect from therapeutic treatment.
- In case of intolerance to the antiulcer drugs used.
- With frequent relapses of the disease.
- For bleeding or perforated ulcers (used in combination with other techniques).
Contraindications
The operation requires preliminary preparation, as well as the absence of contraindications.
These include:
- The patient's serious condition.
- Severe obesity (grade 3-4).
- Infectious and inflammatory processes in the body.
- High risk of blood loss due to blood incoagulability.
- Diseases of the digestive system due to low stomach acidity.
- Zollinger-Ellison syndrome (a tumor of the pancreas that provokes the release of gastric secretions).
- Neurogenic intestinal atony (impaired prostate function of this organ).
In emergency situations, when the patient may die without urgent help, the list of contraindications is not examined.
Preparation
If the operation is planned, preparation is carried out in accordance with the usual protocol, but also includes special studies.
What to do before surgery:
When performing an emergency operation, it is necessary to take into account the need for a possible blood transfusion, the use of solutions that restore blood plasma, as well as resuscitation methods.
Anesthesia and access
The operation involves the use of general endotracheal anesthesia.
Abdominal or thoracic access is implied.
The second option is used for repeated surgical interventions, when the risk of formation of abdominal adhesions is high.
Nowadays, the method of laparoscopy has become increasingly widespread, allowing manipulation with minimal intervention in the body. The recovery period in this case is significantly reduced, as are possible postoperative complications.
The duration of the operation depends on the type of procedure and ranges from two to five hours.
Operation technique
To reduce the risk of possible complications, several techniques for performing such operations have been developed. They are selected individually, depending on the severity of the lesion and the expected benefit for the patient.
Types of vagotomy:
- Trunk surgery involves complete excision of the trunk of the vagus nerve. This is the easiest operation technically, but it may cause serious disruption to the functioning of many internal organs (mainly the gastrointestinal tract).
- Selective vagotomy, in which excision is performed only on the branches leading to the stomach. This reduces the risk of complications in the functioning of the gastrointestinal tract, but is also not a completely safe procedure.
- Selective proximal vagotomy, which is more preferred in modern medicine, involves interrupting signals along the nerve fibers of certain vagal branches. It requires greater precision and skill, and after the procedure all additional functions of the vagus nerve must be preserved, with the exception of acid-producing receptors.
An alternative is drug treatment with a strict diet and special physiotherapeutic procedures.
Reviews
Thanks to timely intervention and compliance with doctors’ recommendations, the prognosis for patients who have undergone gastric vagotomy is quite favorable.
According to reviews and clinical data, complications in the postoperative period occur in only 5-30% of patients, and in most cases, repeated surgery is not required; the problem is solved with drug therapy.
Complications
One of the reasons for the decline in the use of vagotomy is the high risk of complications. These include the appearance of gastric bleeding, perforation or degeneration of an ulcer, or pyloric stenosis.
These conditions are potentially life-threatening for the patient, so vagotomy is now used in emergency cases, when the risk to the patient if not intervened is much greater.
Gastric vagotomy was actively used in the treatment of peptic ulcers in the middle of the last century. Modern development of medicine and the study of the causes of damage to the gastric mucosa have made it possible to develop much more successful methods for treating such diseases.
Now the relevance of using vagotomy is not so high. We are mainly talking about emergency cases, as well as the use in case of ineffectiveness of therapeutic methods of treatment.
Source: https://gidmed.com/gastroenterologiya/lechenie-gastro/hirurgiya/vagotomiya.html
Indications for vagotomy
- Lack of effect from conservative treatment of duodenal ulcer for two years. Now this indication is used less and less, since the effectiveness of new treatment regimens using antibacterial drugs is quite high.
- Intolerance to antiulcer drugs.
- Refusal of the patient from long-term treatment with expensive drugs.
- The disease often recurs despite treatment.
- Perforation of the ulcer.
- Bleeding from a peptic ulcer or erosive gastric mucosa.
Rehabilitation
Vagotomy does not require specific rehabilitation. The principles of recovery that are necessary for the accompanying operation are used. The most important thing is to follow your diet. It is necessary to strictly adhere to the diet after surgery for a perforated gastric ulcer, resection of this organ and gastrectomy.
Advice: you must adhere to the diet for your own good, because violating it can lead to relapse and repeat surgery.
In general, vagotomy is a good treatment for peptic ulcers. But it is worth remembering that the effectiveness of any operation also depends on the qualifications of the surgeon. So, before undergoing surgery, you need to choose the most qualified doctor. And of course, we should not forget the principle that any disease is easier to prevent than to treat.
We recommend reading: gastric resection
Preparation for vagotomy
In planned cases, the usual preoperative preparation is carried out (general tests, biochemical tests, determination of markers of infectious diseases, blood clotting, X-ray of the lungs, electrocardiography, examination by a therapist). Special examinations are carried out:
- Fibrogastroduodenoscopy.
- X-ray contrast examination of the stomach with barium.
- RN-metry.
- Definition of Helicobacter pylori.
In emergency situations, preparation includes stabilizing basic body functions.
- If bleeding occurs, a blood transfusion may be required.
- Infusion of fluids and saline solutions.
- Administration of antibiotics for perforation.
- Installation of a nasogastric tube, aspiration of gastric contents. The probe is left in the esophagus during surgery.
- Installation of a urinary catheter.
Anesthesia, access
This operation uses general endotracheal anesthesia.
Position – lying on your back with the leg end slightly lowered (to move the abdominal organs down). With the abdominal approach, an upper midline incision is made; if necessary, it can extend below the umbilicus and above the xiphoid process. Sometimes the xiphoid process of the sternum can be removed for better access.
For thoracic access, position on the right side. Thoracic access (through the 8-9 intercostal space) is usually used for truncal vagotomy during repeated operations, when adhesions may form in the abdominal cavity.
Truncal vagotomy
truncal vagotomy
After the incision, access is made to the upper floor of the abdominal cavity. The spleen is protected, the left lobe of the liver is mobilized.
The upper part of the stomach is retracted downwards, and the visceral peritoneum above the lower part of the esophagus is incised transversely along its entire length. By blunt tissue dissection, the abdominal esophagus is mobilized.
The left vagus trunk is clearly visible on the anterior surface of the esophagus; it is isolated from the wall of the esophagus using clamps; a 2-3 cm long section is removed between the clamps. The left vagus trunk is duplicated in a third of cases, unlike the right one, so all nerves lying on the surface of the anterior wall must be transected.
The right vagus trunk does not fit tightly to the wall of the esophagus, but is located in the loose tissue surrounding it. It is more convenient to identify it when the esophagus is retracted to the left; it is felt like a stretched string. Clamps are also applied and a section of the barrel is removed.
The completeness of the vagotomy is reviewed. There are so-called criminal branches of Grassi that go to the stomach and can go unnoticed. If they are not crossed, the vagotomy will be incomplete.
The effectiveness of vagotomy
After surgery, peptic ulcer disease can recur. The secretion of acids and the enzyme of the gastric mucosa (pepsin) tends to resume in the same volume over time. 4% of those operated on complain of nausea, bloating, and diarrhea associated with impaired motor function of the gastrointestinal tract. Frequent heartburn, vomiting, belching, and a feeling of premature satiety are signs that reoperation may be required.
Some patients who underwent truncal vagotomy went to medical institutions with gallstones 2-3 years after surgery. Ulcerative relapse most often occurs after stem surgery. Insufficiently complete surgery or failure of the sutures can lead to postoperative hernias.
Sources
- https://medoperacii.com/zhkt/vagotomiya-zheludka.html
- https://operaciya.info/abdominal/vagotomiya/
- https://GastroTract.ru/obsledovanie/tehniki-selektivnoj-i-stvolovoj-vagotomii.html
[collapse]
Selective vagotomy
selective vagotomy
After mobilization of the esophagus, the vagus trunks are isolated, the hepatic branch of the anterior trunk and the abdominal branch of the posterior trunk are identified, they are preserved, and only the gastric nerves of Laterger are excised.
Currently, this type of vagotomy is practically not used; it has been replaced by highly selective vagotomy.
The need for drainage operations
Trunk and selective vagotomy significantly reduce the tone of the stomach walls and disrupt the evacuation of food. In this regard, with these types of vagotomy, drainage operations are necessary, that is, interventions that facilitate the passage of food masses from the stomach to the intestines.
At first it was a gastrojejunostomy, later it was replaced with pyloroplasty according to Heineke-Mikulicz. The main advantages of pyloroplasty:
- This operation is quite simple.
- Provides good drainage.
- More physiological, does not interfere with the gastroduodenal passage of food.
- Pyloroplasty allows you to perform manipulations on the duodenum: revision of the ulcer, suturing of the bleeding ulcer.
Pyloroplasty according to Heineke-Mikulich is an incision in the area of the pylorus and the initial part of the duodenum in the longitudinal direction, and then suturing the hole in the transverse direction. As a result, the pyloric lumen increases, and the evacuation of gastric contents occurs without stagnation.
Usually, vagotomy is performed first, and then pyloroplasty. In emergency situations (bleeding), first access to the duodenum is performed, the bleeding is stopped, then pyloroplasty is performed, and then vagotomy.
Surgeries for stomach ulcers
Depending on the complication that has developed against the background of the ulcer, the following operations are performed:
- Gastrectomy (removal of the stomach, performed when the ulcer becomes malignant);
- Resection (removal of a part, usually 1/3 or 2/3 of an organ, is carried out in case of extensive ulcerative lesions or damage to large vessels);
- Excision of the ulcer (a small area with an ulcerative defect is removed, more often used for perforation of small ulcers);
- Suturing of perforation (for perforated ulcers);
- Suturing a bleeding vessel (for gastric bleeding).
Advice: if there is a choice between suturing the perforation and excision of the ulcer, then you should give preference to the latter option, as it reduces the likelihood of relapse and the formation of a malignant tumor at the site of the ulcer.
Any of these operations creates a fresh wound that will be easily injured by gastric juice. To solve this problem, some doctors prescribe medication, while others perform a gastric vagotomy during surgery.
Selective proximal vagotomy (highly selective)
highly selective vagotomy
The main trunks are isolated, as in the operations described above, the abdominal and hepatic branches are preserved. The greater curvature is retracted down and to the left. Next, the lesser omentum is opened closer to the lesser curvature of the stomach.
The anterior nerve of Laterger stands out and is somewhat extended by the hooks. Lateral branches extend from it, innervating the walls of the stomach. These branches pass as part of the neurovascular bundles. It is necessary to leave 3-4 branches intact that innervate the outlet of the stomach (this is a distance of about 6 cm from the pylorus). Clamps are applied to the remaining neurovascular bundles, they are ligated and dissected.
The surgeon does the same with the posterior gastric nerve.
Once again, the lower part of the esophagus is carefully cleared of nerves, since nerves innervating the stomach may remain.
The peritoneum is sutured.
As a result of this operation, the innervation of the pylorus is preserved, gastric emptying is not impaired and drainage surgery is not required.
Contraindications for selective proximal vagotomy:
- Rough scar-adhesive changes in the lesser omentum.
- Obesity 3-4 degrees.
- Decompensated stenosis.
- Large ulcers of the pyloroduodenal zone with penetration.
Methods of ulcer surgery
Ulcer treatment is carried out according to several schemes. There are stem, selective and selective proximal vagotomy.
Truncal surgery is a process in which the vagal trunk is intersected above the diaphragm area to the site of division of the trunks. Leads to a breakdown of innervation, to disruption of the integrity of connections between organs, tissues and the nervous system. Impossible without subsequent drainage manipulations.
The selective method consists of cutting the gastric branches and preserving their part directed to the hepatic region and solar plexus. An incision is made under the esophageal hiatus of the diaphragm.
The proximal selective method allows you to cross the parts of the vagus directed towards the upper part of the gastric reservoir, thereby preserving the original gastric and alimentary tract to the greatest extent. Proximal vagotomy affects areas containing acid-producing cells. With this type, there is no need to resort to drainage surgery.
Stomach ulcer
Minimally invasive (laparoscopic) vagotomy
Methods of laparoscopic vagotomy, both trunk and selective proximal, have been developed. For this operation, 5-6 punctures are made in the abdominal wall to insert a laparoscope and instruments.
Stages of laparoscopic vagotomy:
- Insertion of a laparoscope, revision of the abdominal cavity, determination of the possibility of laparoscopic VT, choice of method.
- Selection of trocar insertion points.
- Performing the operation itself. The stages of the operation are similar to open vagotomy.
- Restoration of damaged structures.
- Control audit, drainage.
The laparoscopic vagotomy operation is performed under general anesthesia and lasts from 2 to 4 hours. This type of vagotomy has all the advantages of minimally invasive operations (low trauma, short rehabilitation period).
But, despite all the advantages, laparoscopic vagotomy is not yet very common and is not performed in all centers. Carrying it out requires expensive equipment and a highly qualified surgeon, which increases its cost. In addition, since the end of the last century, there has been a decline in interest in vagotomy as a method of planned surgical treatment of peptic ulcer disease, which does not contribute to the spread and improvement of this method.
However, interest in vagotomy is being revived, and the laparoscopic method can become a good alternative to long-term, sometimes lifelong, use of acid-lowering drugs.
Combined and experimental types of vagotomies:
- Posterior trunk plus anterior highly selective vagotomy. The goal is to simplify the technique and save time, the results are similar to bilateral proximal vagotomy.
- Posterior truncal vagotomy with anterior seromyotomy. Seromyotomy is a dissection of the seromuscular layer of the gastric wall at a distance of 1.5 cm parallel to the lesser curvature. The branches of the vagus nerve pass through this area and there are very few blood vessels here.
- Posterior truncal vagotomy with anterior proximal vagotomy using a stapler.
- Cryovagotomy.
- Endoscopic vagotomy using chemicals that destroy nerve fibers.
Postoperative period
Management of patients after vagotomy is not particularly different from the principles of management after any operations on the gastrointestinal tract. The main problems are associated with concomitant operations (pyloroplasty, resection, anastomosis), and not with vagotomy.
A nasogastric tube is left in the esophagus for 4-5 days, and gastric contents are aspirated until the stomach begins to empty on its own.
The patient receives parenteral nutrition for several days, then it is possible to take liquid and semi-liquid food in small portions.
To adapt the stomach to new digestive conditions, it is necessary to follow a diet for about a month, as with an ulcer, with a regimen of frequent split meals.
To monitor the completeness of the vagotomy, a 12-hour overnight study of gastric secretion is performed.
After operation
As soon as the patient recovers from anesthesia, he must be examined by a doctor. He must make sure that the patient is in satisfactory condition. The first day the patient should remain in bed and not eat anything. It is forbidden to turn around and leave the room. Towards the evening you are allowed to drink some liquid. The patient is allowed to roll over.
The next day he can sit on the bed or try to walk around the ward. He is also given a small amount of semi-liquid food. The patient spends approximately a week in this mode. After this, the patient must adhere to a special diet.
If, in addition to vagotomy, pyloroplasty was performed, then in this case, dietary restrictions will be more stringent. The patient needs to adhere to the diet for about 2-3 weeks.
If we talk about the usual procedures, then in the first weeks you need to be extremely careful when performing hygiene measures. If the patient goes into the shower, then after this it is imperative to treat the body with a 5% solution of potassium permanganate. This is necessary in order to prevent the development of infection.