Do you remember the phrase from the film “Ivan Vasilyevich is changing his profession,” when the tsar said menacingly, addressing director Yakin: “Ask the noblewoman for life or death”? In Old Church Slavonic, belly meant life, and if you think about it, this is really true.
Almost all vital organs are located in the stomach, well, of course, with the exception of the brain. Therefore, pain that occurs in the abdomen, especially acute pain, should always be alarming. Our body, with the help of pain impulses, tries to inform the brain about problems, about danger - this is an alarm bell, ignoring which a person exposes himself to a mortal threat.
Types of pain, mechanism of its development
Every tissue in the body contains pain receptors. When damaged, the receptors are irritated, which leads to their excitation, and as a result, pain. There are 2 types of receptors:
- somatic pain receptors, characterized by a high sensitivity threshold; when stimulated, pain occurs;
- visceral polymodal receptors - in case of weak irritation, they transmit information about malfunctions of the organ and only their strong irritation causes pain.
According to the classification of receptors, there are 3 types of abdominal pain or gastralgia:
Somatic pain
There are a lot of somatic receptors located in the parietal peritoneum (covering all the organs of the abdomen like a blanket), in the ureters, mesentery and bile ducts. The intensity of such pain is very pronounced, and the patient accurately determines its location. Accordingly, somatic pain, also known as peritoneal pain, appears when the peritoneum is irritated. Similar pain is observed with a perforated gastric ulcer, intra-abdominal bleeding and other pathologies. Somatic pain is characterized by persistence and in most cases peritoneal symptoms (tension of the abdominal muscles, positive Shchetkin-Blumberg sign, cutting nature, increased pain with movement)
Visceral pain
This pain appears directly in the damaged organ, that is, when receptors located in the walls of the organ are irritated. Visceral pain is painful, dull in nature and is associated either with bloating of the abdominal organs or with their spasm. The patient often finds it difficult to characterize the localization of such pain, since pain is felt not only in the damaged organ (usually the midline of the abdomen) but also in other parts of the abdominal cavity. Clinically, visceral pain manifests itself as colic (renal and hepatic, intestinal and others).
Referred pain
Such pain is a consequence of the irradiation of pain with significant irritation of the affected organ, which is not localized in the abdominal cavity. Referred pain occurs with pathologies of the brain, chest cavity, diseases of the spine or genital organs.
Characteristics of dagger pain in the abdomen
A careful and comprehensive assessment of abdominal pain and observation of the patient provides significant information. Observation of the patient’s behavior and posture during an attack of acute stabbing pain in the abdomen is of great diagnostic importance.
Patients with exacerbation of peptic ulcer disease usually sit or lie hunched over with their legs brought to their stomach. Patients with perforation of gastric and duodenal ulcers usually moan or scream from intense pain, but maintain a forced horizontal position of the same type, since an attempt to change it leads to a sharp increase in pain.
The same situation is typical for patients with local or diffuse peritonitis of various etiologies, with the difference that independent (independent of examination) abdominal pain is usually less intense and patients lie relatively calm.
It should be borne in mind that some people, with the same impulse, experience only a slight unpleasant sensation, others experience a feeling of burning, cutting, nausea, and still others experience unbearable pain. Pain sensitivity increases during menstruation, pregnancy, menopause, and increased nervous activity.
Sharp and constant anxiety of patients with cutting dagger pain, groans or screams, continuous attempts to change body position (horizontal position is replaced by walking, sitting) are very often observed with hepatic and renal colic. These attacks are also characterized by the sudden development and end of acute pain.
The patient's response to pain depends not only on the type and intensity of the lesion, but also on the threshold of sensitivity and on the interpretation of the sensation. Sensitivity to the perception of pain varies from person to person in terms of both intensity and pattern.
Sources:
- https://www.18gp.by/informatsiya/stati/660-bol-v-zhivote
- https://yandex.ru/health/turbo/articles?id=4335
- https://www.5gkb.by/uslugi/napravleniya/khirurgiya/stati/ostrye-boli-v-zhivote/
- https://www.3crkp.by/
The concept of "acute abdomen"
Acute conditions with abdominal pain are traditionally called “acute abdomen” by doctors. This concept was introduced into surgical practice by the famous surgeon Henry Mondor, who by “acute abdomen” meant “abdominal catastrophe” - sharp acute pain requiring prompt medical attention, usually surgical treatment. “Acute abdomen” includes a set of clinical signs, confirmed by laboratory and instrumental data, that occur in acute, life-threatening diseases or injuries/damage to the abdominal, pelvic and retroperitoneal organs. The term “acute abdomen” is not a final diagnosis and is used only in emergency situations until a detailed examination of the patient is carried out and the cause that led to this condition is determined.
To establish the correct diagnosis it is of great importance:
- a correct and carefully collected anamnesis;
- clinical examination;
- X-ray and ultrasound examination of the abdominal organs, as well as the chest;
- CBC, BAM, blood biochemistry;
- laparoscopy.
Acute abdomen clinic
This condition is characterized by a triad of symptoms: acute abdominal pain, tension in the abdominal muscles and impaired intestinal evacuation function, that is, peristalsis. So, the classic signs of an “acute abdomen”:
- sharp cramping pain in the abdomen, appearing periodically or constantly;
- pallor of the skin and mucous membranes;
- gases do not pass, stool is delayed or diarrhea, which indicates a weakening of intestinal motility;
- rapid breathing and pulse;
- decreased blood pressure (typical of intra-abdominal bleeding);
- acute pain is usually combined with nausea and vomiting;
- positive Shchetkin-Blumberg sign (palpation of the abdomen reveals a sharp increase in pain after pressing with fingers on the anterior wall of the abdomen and suddenly withdrawing the hand - the patient’s reaction is determined by the resulting grimace of pain);
- forced position in the “fetal position” - the patient lies on the healthy side, legs are bent and pressed to the stomach, arms and chin are pressed to the chest;
- pain shock;
- acute vascular insufficiency (loss of consciousness) - with internal bleeding or unbearable pain;
- cold sticky sweat, significant weakness and dizziness.
When acute abdominal pain occurs, there is not always an increase in temperature. The clinical picture of an “acute abdomen” without temperature rise is observed with intra-abdominal bleeding (perforation of an ulcer, trauma or gynecological problems: tubal pregnancy, ovarian apoplexy). But in the case of a delayed request for specialized help, the blood that has poured into the abdominal cavity is hemolyzed, its breakdown products are absorbed back into the bloodstream, which leads to aseptic inflammation, the development of diffuse peritonitis and an increase in body temperature. As a rule, an increase in temperature accompanies inflammatory processes in the abdominal and pelvic organs.
Daggering pain in the abdomen is characteristic of
Daggering pain in the abdomen is typical during exacerbation of chronic duodenitis or due to duodenal ulcer disease. “Dagger” pain accompanies ulcer perforation.
Daggering pain in the abdomen is characteristic of gastric ulcer. Peptic ulcer disease can also be the reason that a person experiences dagger pain in the stomach. Pain in this case usually appears in the first half hour or hour after eating. At first the pain is not very pronounced, but as soon as the food begins to be digested, the pain intensifies and becomes unbearable.
Also, stabbing pain in the abdomen is typical when an ulcer perforates. The pathology is expressed in the appearance of a through hole in the walls of the stomach or duodenum, through which the contents of these organs enter the abdominal cavity. The pain is sharp, described as a “dagger blow,” and sometimes causes fainting. The abdominal muscles tense, the general condition suffers. Perforation mainly occurs against the background of stomach and intestinal ulcers.
Dagger-like pain in the abdomen is characteristic of pancreatitis. Pain is the most pronounced symptom, pain with pancreatitis is usually very intense, constant, the nature of the pain is described by patients as cutting, dagger-like. If medical care and pain relief are not provided in a timely manner, the patient may experience pain shock.
Food poisoning can also be a cause of stabbing abdominal pain. The characteristics of clinical manifestations depend on many conditions - the type of microbe or toxin, the amount of food taken, the condition of the body and other factors.
Among the common causes of dagger pain in the abdomen is intestinal obstruction, gastroduodenitis.
What causes acute abdominal pain?
The occurrence of acute abdominal pain is provoked by many reasons. These can be inflammatory diseases of the abdominal, retroperitoneal organs and organs located in the pelvis. Pain syndrome is also characteristic of pathologies accompanied by intra-abdominal bleeding. Abdominal pain can also be caused by diseases of the thoracic cavity and spine.
Acute appendicitis
Perhaps the most common cause of abdominal pain is inflammation of the appendix or acute appendicitis. The onset of the disease is sudden, pain originates in the epigastric region (approximate location of the stomach), then covers the entire abdomen without a specific localization or worries in the peri-umbilical surface. Over time, the pain gradually intensifies, and then descends to the iliac region on the right (with a typical location of the appendix). The temperature gradually increases (subfebrile, not higher than 38 degrees), the pulse quickens, signs of intoxication-inflammatory syndrome appear (the tongue is dry and coated - “like a brush”, weakness, loss of appetite, nausea, possible vomiting). Palpation of the abdomen allows one to determine sharp pain in the right side, peritoneal symptoms (positive Shchetkin’s sign, muscle tension). The subsidence of the pain syndrome is considered a very unfavorable sign and indicates its transition to the gangrenous stage, when the nerve endings of the appendix die. Gangrene of the appendix is fraught with perforation and the development of diffuse peritonitis. Read more about the symptoms of appendicitis.
What to do : Call a local doctor or an ambulance. Taking painkillers is prohibited.
Acute intestinal obstruction
In case of intestinal contents evacuation disorder, intestinal obstruction develops. There are 2 known forms of this pathology: dynamic (as a result of intestinal spasm or paresis) and mechanical (a plug is formed in the intestine, represented by a foreign body, a clot of helminths, a gallstone, or tugging of an intestinal loop with adhesions). Infringement or compression of the intestinal loop can be provoked by heavy physical work associated with tension in the abdominal muscles, constipation or errors in diet. Intestinal volvulus (torsion) is a consequence of adhesions and excessive length.
This pathology begins with sudden acute pain in the abdomen, the nature of which is cramping, and the intensity varies. Pain in the form of spasms is characteristic of the obstructive form of obstruction (calculi, tumor, helminths, etc.). In the case of intestinal strangulation (compression by adhesions, torsion or strangulation of a hernia), the pain syndrome is constant and very intense - the patient groans and screams. Intestinal obstruction is always accompanied by pain, which is the leading diagnostic sign. If you do not consult a doctor in a timely manner, the pain gradually decreases and disappears, which is associated with necrosis of the nerve endings and the damaged intestinal loop itself. In this situation, diffuse peritonitis develops, vomiting occurs, the tongue is “like a brush,” peritoneal symptoms of the abdomen are noted in all its parts, pain in the abdominal wall upon palpation, stool and gases do not pass away.
What to do : Immediately call an emergency team; you can take an antispasmodic (don’t forget to tell your doctor about this). Do not take laxatives or do an enema under any circumstances.
Strangulated hernia
Hernias are classified as congenital or acquired, which appear in “weak” areas of the abdomen. There are also postoperative hernias that form in places of postoperative scars. The provoking factors of infringement are a sharp increase in internal abdominal pressure, which occurs after heavy physical labor and heavy lifting, screaming and crying of a child, a prolonged period of straining, constipation, coughing and sneezing, and so on.
Pain from strangulation is localized at the location of the hernia (in the groin or femoral region, in the navel or postoperative scar). The pain syndrome is characterized by intensity, occurs against a background of nausea and vomiting, stool and gas are retained, and the heartbeat increases. At the site of the hernia, the patient feels a dense and very painful formation (round or oblong), which cannot be reduced into the abdominal cavity. If you do not seek medical help in a timely manner, necrosis of the strangulated organ, usually the intestinal loop, and peritonitis develops.
What to do : immediately call an ambulance; before the call, you can take antispasmodics.
Perforated ulcer
The appearance of abdominal pain can be caused by perforation of hollow organs, which often complicates gastric and/or duodenal ulcers. A very characteristic sign of perforation of an ulcer is “dagger”, that is, sudden and very sharp pain. The pain syndrome is persistent and severe. The victim takes a forced position and tries not to move and hold back his inhalations and exhalations. In the first hours of complications, pain is felt in the epigastric region and under the ribs on the right. If the perforation is not covered by an intestinal loop or omentum, the pain quickly covers the entire abdomen. The pain can radiate to the right shoulder and spine, under the scapula and collarbone. The second cardinal sign of a perforated ulcer is a sharp tension (hardening) of the abdominal muscles, the abdomen retracts and cannot be palpated. Surgeons compare this condition to a board (the abdomen is hard like a board). Read more about the symptoms of stomach ulcers.
What to do : Call 03 immediately. The patient is prohibited from eating and drinking.
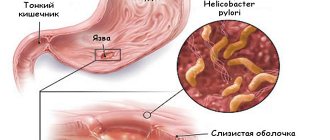
Acute gastritis
The cause of the disease is Helicobacter bacteria. Errors in the diet (spicy, fatty foods) or stress can provoke excessive release of hydrochloric acid. With long-standing gastritis, there is a high risk of developing peptic ulcers. But gastritis is also isolated with low acidity, in which hydrochloric acid is not produced in sufficient quantities, which promotes the proliferation of Helicobacter pylori, delays the digestion of food in the stomach and leads to its rotting. With gastritis, the pain is localized in the pit of the stomach (in the epigastrium), characterized by significant intensity, sharp and constant. Periodically occurring acute pain is associated with the action of provoking factors. Read more about the symptoms of gastritis.
What to do : Contact your local doctor, consult a gastroenterologist, undergo an FGDS.
Peptic ulcer: exacerbation
Exacerbation of a stomach/duodenal ulcer is characterized by sharp abdominal pain that occurs a few minutes (10–30) after eating. At the peak of a painful attack, profuse vomiting of acidic contents is possible. Often the pain occurs at night or on an empty stomach and subsides after a snack. The pain is localized in the epigastrium; less often, acute pain occurs in the right side of the abdomen (right hypochondrium). Irradiation of pain occurs in the lumbar region, chest, and sometimes in the lower abdomen. The pain syndrome intensifies with physical activity, and the attack decreases in a stationary and forced position. Pain during an exacerbation of an ulcer often occurs against the background of heartburn and vomiting, but the appetite does not suffer, although there is a fear of eating.
Chronic enteritis: exacerbation
This disease occurs as a result of inflammation and dystrophic changes in the mucous membrane of the small intestine, often combined with damage to the large intestine (enterocolitis). The causes are previous intestinal infections or giardiasis. The clinical picture is represented by a dull aching pain, which is not sharply expressed and appears either after eating or has no connection with eating. The patient also complains of distension in the epigastric and periumbilical region and fullness, heaviness, loss of appetite, bloating/rumbling in the abdomen. Upon examination, dry skin, brittle nails, and bleeding from the gums (polyavitaminosis) are revealed.
What to do : consultation with a gastroenterologist.
Chronic colitis: exacerbation
When this disease worsens, minor pain occurs in the lower half or throughout the abdomen. There is also heaviness in the abdomen, burning and itching in the anus, the patient complains of bloating and rumbling, and palpation of the abdomen reveals pain along the large intestine.
What to do : consult a gastroenterologist, follow a diet.
Hepatic colic
An attack of hepatic colic is a consequence of blockage of the neck of the gallbladder by a stone, or blockage of its ducts by a stone in case of cholelithiasis or acute inflammation of the gallbladder (cholecystitis). A painful attack due to gallstones is caused by a violation of diet, physical and nervous overload. The pain occurs unexpectedly and is very sharp, quickly increases and is felt in the right hypochondrium and epigastrium. The pain radiates under the right collarbone and scapula, into the right shoulder and the right half of the neck. Rarely, pain radiates to the lower back and iliac region. When lying on the left side, the pain also increases during inhalation, which is caused by tension in the peritoneum. An attack of severe pain can last several days. The patient is also concerned about constant nausea and vomiting of bile without relief. On examination, yellowness of the skin and sclera is noted. The temperature rises, an increase in leukocytes and neutrophils is detected in the blood.
What to do : Call a doctor immediately and refuse to eat until hospitalization.
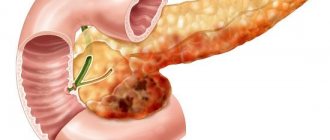
Acute pancreatitis
Inflammation of the pancreas is provoked by liver pathology, diseases of the bile ducts and other organs involved in digestion, a passion for fatty, fried and spicy foods, alcohol abuse, as well as injuries and surgeries, allergies and other factors. The patient feels pain in the upper half or left side of the abdomen. In most cases, the pain is girdling. The pain syndrome is long-lasting, characterized by painfulness and squeezing/drilling. Periodically, the acute pain decreases, but disappears completely. Against the background of pain, abdominal bloating and painful, sometimes uncontrollable vomiting occur. Possible loose stools and yellowness of the sclera. Read more about the symptoms and treatment of pancreatitis.
What to do : The golden rule of surgeons for acute pancreatitis: cold, hunger and rest. Call 03.
Acute diverticulitis
Meckel's diverticulum is a saccular protrusion of the wall of the small intestine, which is formed against the background of incomplete fusion of the vitelline duct. Often diagnosed in childhood. Characterized by intestinal bleeding, blood found in the stool (melena) and symptoms of intestinal obstruction. The pain is very intense, located to the right of the navel or slightly lower.
What to do : immediately call an ambulance, as the disease requires emergency surgery.
Renal colic
An attack of renal colic is characterized by a sudden onset, the pain is sharp and excruciating, located in the lower back, “descends” along the ureter and radiates to the perineum, groin and leg. The pain syndrome is also combined with dysuric symptoms (painful and frequent urination, hematuria), nausea, flatulence and vomiting.
If there are stones in the kidneys and/or ureters, a painful attack occurs without a specific reason. In case of nephroptosis after physical activity, heavy lifting or long walking. In addition, the attack can be caused by a blood clot in the urinary tract. The pain lasts for several hours. In some cases, pain is felt in the lower abdomen or iliac region. A painful attack is very similar to the picture of an “acute abdomen”: nausea and vomiting, gases and stools do not pass, weakened peristalsis, increased temperature, etc. Patients are often hospitalized in the surgical department. The patient's restless behavior is considered characteristic of renal colic; he rushes about and cannot stay in bed. The attack may end suddenly. Read more about the symptoms and treatment of renal colic.
What to do : seek medical help as quickly as possible; taking antispasmodics and taking a warm bath is allowed, provided that the patient knows that he has kidney stones.
Diseases of the chest organs
Pathology of the thoracic cavity organs is often accompanied by abdominal pain:
- myocardial infarction;
- lower lobe right-sided pneumonia (lobar);
- inflammation of the pleura, which covers the chest from the inside) - pleurisy;
- failure of the right ventricle of the heart (blood stagnates in the systemic circulation, which leads to its accumulation in the liver, legs and other organs);
Abdominal syndrome during myocardial infarction is characterized by acute pain in the epigastric region, and occurs with nausea and vomiting. The pain is bursting or pressing in nature and is combined with characteristic signs of the disease:
- atrial fibrillation;
- drop or jump in blood pressure;
- anxiety and fear of death and so on.
Right-sided pneumonia is accompanied by pain in the upper right part of the abdomen, and signs of peritoneal irritation may appear. A distinctive feature of the pain syndrome is its development against the background of symptoms of acute pulmonary inflammation:
- high temperature (38 and above);
- dyspnea;
- on auscultation, weakened breathing in the affected lobe of the lung;
- the chest on the right is behind in breathing and other signs.
Inflammation of the pleura is also accompanied by pain in the upper abdomen. Pain intensifies with coughing and deep sighs.
Right ventricular failure is characteristic of mitral stenosis. Pain occurs under the ribs on the right, which is caused by an enlarged liver (hepatomegaly). The pain is dull, aching.
Example from practice : Once I was on duty in the ambulance, essentially performing the functions of an emergency room doctor. They brought a mother and a boy about 9 years old. The mother complained of acute abdominal pain in the child. The pain started a few hours ago. Temperature 37.5. The boy and mother did not make any other complaints. During auscultation of the lungs, I did not hear anything pathological. Palpation of the abdomen is painful, peritoneal symptoms are weakly positive, the abdomen is soft. The tongue is wet and coated. There is no nausea or vomiting. She called a surgeon for a consultation (a child with a suspected “acute abdomen”). The surgeon, after listening to the lungs, made a diagnosis: “right-sided lower lobe pneumonia” and sent the patient for an X-ray examination.
Intestinal infections
Acute abdominal pain also accompanies intestinal infectious diseases. The intensity of pain and intoxication syndrome is determined by the causative agent of the infection.
Acute dysentery (inflammation of the large intestine, rectum) is characterized by the appearance of cramping pain in the lower abdomen, more on the left, and is accompanied by diarrhea. Diarrhea is severe, stools are very frequent, up to 20 times a day, and quickly lose their fecal character. The cardinal sign of dysentery is “rectal spitting” - the urge to defecate is frequent and painful with the release of a lump of mucus and pus with blood streaks.
Salmonellosis occurs with damage to the large and small intestines. Acute abdominal pain that occurs with this disease is not clearly localized, often diffuse throughout the abdomen. A distinctive sign of salmonellosis is loose and frequent stools, and the stool has a dirty green color (“swamp mud”).
With viral intestinal infections, pain is localized in the navel area, spastic in nature and accompanied by vomiting, but copious and rare stools.
What to do : call your local doctor, do not refuse hospitalization.
Diseases of the female genital organs
Acute pain in the lower abdomen in women, as a rule, accompanies inflammatory processes of the internal reproductive organs (uterus, tubes, ovaries). Pain is felt in the lower abdomen (iliac regions) and is accompanied by intoxication syndrome (weakness, fever alternating with chills, loss of appetite, dizziness). In acute endometritis, pain is localized above the pubis and in the lower half of the abdomen. The disease develops rapidly, the temperature rises sharply (up to 39 degrees), and the general condition suffers. There is purulent discharge mixed with blood - “meat slop”, which has an unpleasant odor.
With inflammation of the uterine appendages, the pain is located in the lower abdomen, in both iliac regions (bilateral adnexitis) or on the right/left. The pain is described as sharp or aching, constant and radiating to the lower back, sacrum, and perineum. Symptoms of intoxication are also present.
Intra-abdominal bleeding caused by gynecological pathology (ovarian rupture or ectopic pregnancy) is also accompanied by pain. During an ectopic pregnancy, the pain is periodic and cramping and is accompanied by slight or moderate bleeding from the genital tract. The described clinic is typical for tubal abortion. In the event of a pipe rupture, a woman feels a very sharp and sudden pain on the right or left in the groin, there is a rapid drop in blood pressure and increased heart rate (blood quickly fills the abdominal cavity), pale skin, and possible loss of consciousness.
What to do : if you suspect an ectopic pregnancy, immediately call an ambulance, and put the patient in bed and put cold on the lower abdomen. Cold is also necessary for inflammation of the genital organs. The patient needs to see a gynecologist.
Diseases of the male genital organs
Acute abdominal pain in men often occurs due to inflammation of the prostate. Acute prostatitis can be provoked by urethritis, as an ascending infection, sexual dysfunction (violent or infrequent sexual activity, interrupted sexual intercourse), physical inactivity, sedentary work, constipation, alcohol, etc. The pain is felt behind and above the pubis, radiating to the sacrum and groin, to the perineum and lower back, to the rectum. The pain is also combined with frequent and painful urination, fever, weakness and decreased performance. Stool disorders (diarrhea, painful bowel movements) cannot be ruled out; then the pain becomes unbearable and pulsating and is felt in the rectum.
Possible disease based on pain location
Depending on the location of the pain, a possible pathology can be assumed:
Pain in the right hypochondrium
- pathology of the lungs and chest organs (lower lobe pneumonia on the right, pulmonary infarction, fractures of the lower ribs on the right, pulmonary embolism - PE);
- liver diseases (acute hepatitis, hepatomegaly, benign and malignant tumor formations, liver abscess, liver injury);
- diseases of the biliary tract (acute or chronic cholecystitis with hepatic colic, cholelithiasis, biliary dyskinesia);
- gastric pathology (exacerbation of stomach ulcers, acute and chronic gastritis, perforation of gastric ulcers, acute dilatation of the stomach - overeating);
- diseases of the duodenum (exacerbation of duodenal ulcer, perforation of duodenal ulcer, acute pancreatitis or pancreatic cancer);
- kidney disease (acute and chronic pyelonephritis, renal colic due to urolithiasis);
- heart disease (pericarditis, angina pectoris, acute myocardial infarction, right ventricular heart failure);
- intestinal pathology (retrocecal appendicitis - atypical location of the appendix);
- other causes are herpetic infection in the form of herpes zoster or subdiaphragmatic abscess.
Pain in the pit of the stomach (in the epigastrium)
- cardiac pathology (abdominal myocardial infarction syndrome, pericardial inflammation);
- pathology of the esophagus (esophagitis - inflammation of the esophagus, hiatal hernia, perforation of the esophagus);
- pathology of the stomach (acute and chronic gastritis, peptic ulcer of the stomach and duodenum, achalasia of the cardia);
- diseases of the pancreas (acute inflammation or tumors of the gland);
- other causes (sternum injury - fracture or costochondritis).
Pain in the left hypochondrium
- lungs, chest (fractures of the lower ribs on the left, left-sided lower lobe pneumonia);
- pathology of the spleen (splenomegaly, trauma or abscess of the spleen, aneurysm of the splenic artery);
- gastric pathology (gastritis, stomach cancer or benign tumors, exacerbation of a stomach ulcer; perforation of a gastric ulcer, acute pancreatitis, malignant lesion of the tail of the pancreas, pancreatic cysts);
- for kidney diseases (renal colic or pyelonephritis).
Pain in the navel area
- the pancreas is affected (in the case of tumors or pancreatitis);
- the intestine is affected (in case of mechanical intestinal obstruction, early stage of appendicitis, in case of thrombosis of mesenteric vessels or intestinal infarction, in case of strangulation of the inguinal hernia, umbilical hernia, diverticulitis, enteritis and volvulus of the greater omentum);
- other etiology (uremia, leukemia).
Pain in the right iliac region
- intestinal pathology (in acute appendicitis or mesadenitis, strangulation of a right-sided inguinal hernia, perforation of the cecum caused by a tumor, foreign body or diverticulitis, perforation of a gastric or duodenal ulcer);
- kidney pathology (pyelonephritis or renal colic);
- diseases of the female reproductive organs (acute adnexitis: tubo-ovarian formation, pyovar, pyosalpinx, ectopic pregnancy and ovarian rupture, pain during ovulation and endometriosis, torsion of the pedicle of the ovarian cyst);
- vascular diseases (iliac artery aneurysm).
Pain in the left iliac region
- intestinal pathology (diverticulitis of the sigmoid colon, perforation of the descending colon, strangulation of the left-sided inguinal hernia);
- pathology of the female genital organs (acute inflammation of the appendages and ectopic pregnancy, endometriosis and torsion of the pedicle of the ovarian cyst);
- kidney damage (pyelonephritis or renal colic).
Other etiology
Left iliac artery aneurysm, ruptured abdominal aortic aneurysm, or psoas abscess.
Dagger pain in the stomach
Abdominal pain is one of the most common reasons for seeking emergency medical care and, in some cases, one of the symptoms of acute surgical diseases of the abdominal organs (acute appendicitis, perforated gastric ulcer, intestinal obstruction, etc.), requiring emergency referral of the patient to the surgical department .
Abdominal pain is one of the most common reasons for seeking emergency medical care
Determining the nature of abdominal pain greatly contributes to correct diagnosis. It is necessary to find out whether the pain began suddenly or increased gradually. Thus, sudden, acute, so-called dagger-like pain in the abdomen is observed with perforation of ulcers of the stomach and duodenum.
The sudden nature of dagger pain in the abdomen is characteristic of some types of acute intestinal obstruction (intestinal volvulus, strangulation, nodulation). Suddenly, acute dagger pain in the abdomen begins with acute pancreatitis, thrombosis of intestinal vessels, rupture or torsion of ovarian cysts in women.
The sudden development of acute stabbing pain is extremely characteristic of hepatic and renal colic. Pain syndrome increases less acutely with intestinal obstruction; a gradual increase in acute stabbing pain is also characteristic of acute inflammatory diseases (acute appendicitis, cholecystitis, inflammation of the uterine appendages).
Helping the patient before the doctor arrives
If acute abdominal pain occurs, the victim should be given first (pre-medical) aid, and the sooner the better. Anyone who has experienced acute abdominal pain in themselves or a loved one should know the basic rules of behavior in such a situation:
- first of all, the patient should be put to bed and ensure rest;
- find out whether the sick person has any chronic diseases of the digestive system, whether similar situations have happened in the past, and what measures he took to alleviate the condition;
- immediately call an emergency team in case of abdominal injury (the pain is very significant, there is nausea and vomiting, especially with blood), the appearance of black stools, acute urinary retention and detection of bloody streaks in the urine or vomit;
- It is allowed to take antispasmodics (no-spa, papaverine), which should be reported to the doctor;
- apply ice or a bubble of cold water to your stomach;
- in case of absence of consciousness and preserved pulse and breathing, the patient should be placed on his stomach, turning his head to the side (this position ensures free breathing and prevents suffocation or inhalation of vomit and its penetration into the lungs);
- If there is no breathing or pulse, place the victim on a hard surface and begin primary resuscitation (artificial respiration and chest compressions).