Examination of the stomach has always been a difficult task. In order to assess the condition of the mucous membrane and have the most complete understanding of the function of the stomach and duodenum, gastric probing is performed. What is this diagnostic method? How to prepare for the procedure? What are the indications and contraindications for sounding? The answers to these questions can be found by reading the following article.
What is sounding and who is it prescribed for?
The contents of the stomach and duodenum are aspirated using a probe and then examined in the laboratory, where the pH of gastric juice is determined by titration method. Determining the acidity of gastric juice is important when prescribing drug therapy. The study is carried out fractionally, first on an empty stomach, then after 15 minutes and after stimulation.
The procedure involves inserting a tube through the patient's mouth or nose, which is then advanced into the stomach. This examination does not cause discomfort, although it is performed without anesthesia.
Modern medicine has made it possible to use a very thin probe with a diameter of 0.5 cm for this procedure. That is why probing does not bring any unpleasant sensations. In addition, now one end of the probe is equipped with a small video camera, which displays a picture on the monitor screen about the condition of the stomach and its structure.
Content:
- What is sounding and who is it prescribed for?
- Preparation for the procedure
- How is probing carried out?
- Interpretation of survey results
- Contraindications to undergoing the examination
- Recovery after the procedure
- Summing up
This diagnostic method allows the doctor to more accurately diagnose the patient, detect and prevent the development of various diseases.
With the help of gastric probing, diseases such as stomach ulcers, reflux esophagitis and gastritis with low or high acidity can be detected in the early stages.
In addition, this procedure is used for other purposes. Often, a probe is used to introduce medications or food directly into the stomach of a patient who cannot do this themselves: premature babies, patients with injuries to the esophagus, face, oral cavity or pathologies of the larynx, unconscious patients.
Probing is also often used in medical practice for aspiration of poisons and toxins from the stomach in case of toxic damage. A special type of probe is used for this.
This type of diagnosis also makes it possible to identify malignant neoplasms in the early stages and prevent their development, signal any changes occurring in the gastric tissues, and also learn about the structural features of the mucous membrane.
Endoscopic mucosal resection (EMR)
The EMR technique was developed by Japanese scientists for the treatment of superficial cancers. Its great advantage is the possibility of obtaining an entire formation for subsequent morphological research. After identifying the lesion using endoscopic ultrasound and chromoscopy/fluorescence, the lesion is elevated by submucosal injection of saline with or without epinephrine. Some researchers advocate the use of mucopolysaccharide for submucosal administration due to its slower diffusion [18]. In the esophagus, an injection of 5 ml of solution is sufficient; in the stomach and colon, more is usually required [19]. Cutting off at the level of the submucosal layer is carried out using a transparent nozzle, an endoscopic tube for resection of the esophageal mucosa or a two-channel endoscope [20]. The whole specimen is then removed for morphological examination. Complications including bleeding, perforation and emphysema occur in 3-13% of cases [21. Fortunately, complications can be treated endoscopically in most cases.
Preparation for the procedure
The most important thing before carrying out such a procedure is to calm down and put your nervous system in order. Excessive anxiety and nervousness will only negatively affect gastric juice and cause an unwanted gag reflex.
Before diagnosis, it is recommended to talk with your doctor about exactly how the examination will take place, tune in to a positive effect and stop worrying.
In addition, before probing, it is necessary to refrain from eating any food and smoking for twelve hours, so as not to disturb the composition of the gastric juice. You can still drink water.
If the patient is taking any medications, he must notify the doctor who will conduct the examination. Before this procedure, it is not recommended to use antacids, caffeine, atropine and other medications that affect the functioning of the stomach.
Next, the patient is prepared for the procedure directly in the doctor’s office. To do this, he lies down on his left side and covers his chest with a napkin so as not to stain his clothes with saliva. Saliva is spit out during diagnosis; it is not allowed to swallow it.
A special ring is inserted into the patient’s mouth, which will prevent him from closing his jaw and accidentally damaging the probe. The oral cavity is treated with an anesthetic aerosol to reduce sensitivity.
The probe is inserted directly behind the root of the tongue, and then the patient, using swallowing movements, pushes it deep into the stomach. Afterwards it is fixed on the patient’s clothes so that it does not slip deeper.
The free end of the probe is connected to a special pump, which will be used to aspirate the contents of the stomach.
Nasogastric feeding tube “Apexmed International BV”, Netherlands
Made from transparent polyvinyl chloride, implantation-free and non-toxic. The Apexmed feeding probe has an atraumatic terminal end and a radiopaque line.
Label location:
Length 1200 mm: 500 mm, 600 mm, 700 mm, 800 mm, 900 mm from the distal end;
Length 400 mm: 150 mm, 160 mm, 170 mm from the distal end.
Sterilization: ethylene oxide.
Single use.
Shelf life: 5 years
Instructions for use:
- measure the distance from the tip of the nose to the earlobe, mark this distance on the probe (1st mark);
- measure the distance from the incisors to the navel plus the width of the patient’s palm, mark it on the probe (2nd mark - “entrance to the stomach”);
- lubricate the probe with sterile glycerin or sterile vaseline oil;
- insert the probe through the nasal passage first to a distance of up to 1 mark;
- then, making sure that the probe is at the root of the tongue, continue inserting the probe up to the 2nd mark;
- make sure that the probe is in the stomach (auscultation of the epigastric region after introducing 20 ml of air into the stomach through the probe);
- secure the free end of the probe to the patient’s cheek using an adhesive plaster or a special set;
- connect a syringe or enteral nutrition system with a nutritional mixture to the probe cannula;
- at the end of feeding, rinse the probe with 30-50 ml of water;
- Before the next administration of the nutritional mixture, close the end of the probe with a special plug and attach it with a plaster on the cheek;
- remove the probe through a napkin moistened with a disinfectant solution;
- process and dispose of the probe in the prescribed manner.
Manufacturer: Аpexmed International BV , Netherlands (Apexmed)
| Ch/Fr | Inner diameter ID (mm) | External diameter OD (mm) | Color coding | Length 400 mm, Price | Length 1200 mm, Price |
| 4 | 0,8 | 1,4 | red | RUB 23.00 | 19.50 rub. |
| 5 | 0,9 | 1,7 | yellow | ||
| 6 | 1,1 | 2,0 | blue | ||
| 8 | 1,7 | 2,7 | blue | ||
| 10 | 2,3 | 3,3 | black | ||
| 12 | 2,8 | 4,0 | colorless | ||
| 14 | 3,3 | 4,7 | |||
| 16 | 3,8 | 5,3 | |||
| 18 | 4,5 | 6,0 |
How is probing carried out?
This diagnostic method takes quite a long time and can last up to two and a half hours. This depends on the condition of the patient and on the procedure used.
It is usually carried out in a standard way:
- First, all its contents are aspirated from the stomach.
- Then, every 10 minutes for an hour, the secretion produced by the stomach on an empty stomach is collected. The fluid collection time is five minutes.
- Afterwards, a so-called test breakfast is introduced into the stomach. This could be cabbage broth, light broth, or medicinal secretion stimulants: insulin, pentagastrin or gestamine. These drugs have their own contraindications for use, so a trial breakfast is now practically not carried out. In addition, it does not give the desired stomach reaction.
- Half an hour after the introduction of breakfast, they again begin to select the secretion caused by irritants. The collection is also carried out within an hour in fifteen-minute portions.
Each portion of liquid received is tested in the laboratory. It is assessed for smell, appearance and consistency. Pay attention to the total amount of content received.
The importance of staging
Lymph node involvement is directly related to the T stage of the lesion. Folli et al [22] conducted a multicenter, retrospective study of 584 patients with early gastric cancer who underwent D1 gastrectomy. Only 3.7% with lesions limited to the mucosa had metastases to the lymph nodes, while when the submucosal layer was involved, metastases were observed in 25.3%. Shimada et al [23] conducted a retrospective study of 1051 patients with early gastric cancer who underwent gastrectomy with D1 or D2 lymph node dissection. The incidence of lymph node metastases was 2.3% for tumors limited to the mucosa and 19.8% for tumors involving the submucosal layer. Tumors limited to the mucous membrane that had metastases to the lymph nodes were ulcerated. The authors concluded that all patients with tumor confined to the mucosa and without ulceration should be considered candidates for EMR. In addition to the nature of the tumor surface, the boundaries from the edges of the specimen to the tumor cells are important [24]. Japanese researchers have shown [25] that the recurrence rate is 0% when the margin is 2 mm or more, 20% when the margin is less than 2 mm, and 50% when tumor cells are present at the margins of the specimen.
According to the Japanese Association of Gastrointestinal Endoscopy, the absolute indication for EMR is superficial esophageal cancer type IIa, IIb, or IIc, tumor size less than 2 cm, and intraepithelial cancer - m1 cancer. For early gastric cancer, the tumor must be elevated (type I or IIa), confined to the mucosa, well differentiated and less than 2 cm in size in type I and well differentiated, less than 1 cm in size and without ulceration in type IIa. There is no consensus on broader indications for mucosal resection [26].
Esophagus
Fujita et al [27] studied 150 patients with superficial squamous cell carcinoma of the esophagus who underwent EMR or esophagectomy. Of the 72 patients who had tumors limited to the mucosa, 35 patients underwent EMR and 37 patients underwent esophagectomy. The complication and mortality rates in patients after EMR were lower than after esophagectomy (7% to 69% and 0% to 14%, respectively). Long-term survival with EMR was the same as with esophagectomy. The analysis showed that the duration of survival did not depend on the type of treatment - mucosal resection or esophagectomy - in patients with tumors limited to the mucosa.
Takeo colleagues [28] studied the use of an EMR tube in 29 patients with esophageal cancer limited to the mucosa (27 patients with 33 lesions) or dysplasia (2 patients with two lesions). Twenty of the 35 lesions were resected en bloc, and 15 were removed using the lump technique. 10 patients with 15 lesions were diagnosed with m3 cancer or its more invasive types, 5 patients in this group underwent surgery. Of the remaining 24 patients, not one died from esophageal cancer with an average follow-up of 30.9 - 18.9 months. Four-year survival in the EMR group was 100% for m1-m2 tumors, 75% for m3 tumors, and 100% in the surgery group.
Buttar colleagues [29] combined EMR and photodynamic therapy in patients with esophageal cancer arising from Barrett's esophagus. Seventeen patients with proven stage T1 lesions underwent mucosal resection followed by photodynamic therapy after 4 weeks, which was repeated if necessary. In 16 patients, histological and clinical remission was observed at an average follow-up of 13 months. One patient underwent surgery due to the presence of an invasive tumor.
Stomach lesions
Ono et al [30] performed EMR on 445 patients with superficial gastric lesions. For pathological processes limited to the mucosa, complete resection (i.e. when the margins of the specimen were free of pathological cells) was performed in 69% (278/405), while resection was incomplete in 31% of cases (127/405). The relapse rates were 2% and 17%, respectively. There were no gastric cancer-related deaths observed at a mean follow-up of 38 months. In all cases of relapse, radical interventions were performed.
Yoshikane et al [31] investigated the feasibility of performing endoscopic aspiration mucosal resection by nipping for larger superficial intramucosal gastric tumors. All five patients had stomach cancer measuring 4 cm or larger (mean size 4.8 cm). Endoscopic aspiration resection of the mucosa was performed by biting using a panendoscope with an attachment. During an observation period of 16.4 ± 1.1 months, residual tumor (or its recurrence) was detected in one patient, and no tumor was observed in 4 patients.
Suzuki et al [32] recently developed a new endoscopic technique involving endoscopic full-thickness resection and complete endoscopic closure of the defect in the treatment of one duodenal lesion and two cases of rectal carcinoid. The method makes it possible to perform a wider and deeper resection. In addition, it has been demonstrated that EMR, using a high-frequency probe and under endoscopic ultrasound guidance, can be successfully used to remove small submucosal tumors of the gastrointestinal tract [33].
Interpretation of survey results
This procedure is aimed mainly at studying the secretory function of the stomach. It can be used to diagnose most diseases of the digestive system:
- a clear, non-viscous liquid with normal acidity indicates a completely healthy stomach;
- the predominance of yellow or green in the liquid indicates an admixture of bile, red and brown - an admixture of blood;
- food residues in the pumped out fluid and an increased total volume make it possible to judge hypersecretion of gastric juice;
- increased fluid viscosity indicates the presence of gastritis;
- depending on the content of hydrochloric acid, treatment is directed either to limit its production, or, conversely, to stimulate it;
- the acidity of the stomach is established: low or high.
Nasogastric feeding tube TRO-NUTRICATH and children's (pediatric) TRO-NUTRICATH paed
Nasogastric feeding tube for children TRO-NUTRICATH paed - is a hollow tube equipped with a sealed Nelaton type tip with two side holes and
connector for connecting to dosing devices. The nasogastric tube is intended for enteral nutrition and administration of medications into the gastric cavity. Can be used in neonatology, pediatrics and adult patients.
Properties and advantages of the TRO-NUTRICATH probe and TRO-NUTRICATH paed: - made of neutral polyvinyl chloride (PVC), which allows the probe to be used for three weeks without deteriorating their properties, without allergic reactions; — the rounded, soft end of the probe ensures easy, atraumatic and painless insertion. — the presence of side holes at the end contributes to the fullest possible flow of nutritional mixtures and drug solutions into the stomach, sufficient drainage of the stomach and reduces the risk of developing dumping syndrome; — the connector is equipped with a hermetically sealed plug that prevents the leakage of liquid and prevents infection of the contents of the probe; — the probe connector has an adapter, thanks to which the nasogastric tube is compatible with devices of two types of connection: Luer and Catheter-type (with standard-volume syringes, large-volume syringes, automatic dosing devices); — a radiopaque strip along the entire length, and marks every 10 cm, make it easier to determine the position of the catheter in the gastrointestinal tract; — the connector is color-coded depending on the size of the nasogastric tube (in accordance with ISO standards), which makes it easy and quick to select the required size; — Size range: NUTRICATH paed — 4-10 Fr (length 50 cm) NUTRICATH — 6-24 Fr (length 105 cm); — sterile individual blister packaging (paper + plastic film).
Shelf life: 5 years
Manufacturer: TROGE MEDICAL GMBH, Germany (Remains)
Size chart Nasogastric feeding tube for children (pediatric) TRO-NUTRICATH paed:
| Ch/Fr | External diameter OD (mm) | Inner diameter ID (mm) | Length, (cm.) | Color coding | Price including VAT (RUB) |
| 4 | 1,3 | 0,72 | 50 | red | 20,00 rub. |
| 5 | 1,7 | 1,07 | grey | ||
| 6 | 2,0 | 1,26 | green | ||
| 7 | 2,3 | 1,5 | burgundy | ||
| 8 | 2,7 | 1,87 | blue | ||
| 9 | 3,0 | 2,0 | orange | ||
| 10 | 3,3 | 2,25 | black |
Size chart for adult nutritional probe TRO-NUTRICATH:
| Ch/Fr | External diameter OD (mm) | Inner diameter ID (mm) | Length, cm | Color coding | Price |
| 6 | 2,0 | 1,05 | 105 | St. green | RUB 23.00 |
| 8 | 2,67 | 1,5 | violet | ||
| 10 | 3,33 | 2,0 | black | ||
| 12 | 4,0 | 2,45 | white | ||
| 14 | 4,67 | 2,95 | green | ||
| 16 | 5,33 | 3,4 | orange | ||
| 18 | 6,0 | 3,9 | red | ||
| 20 | 6,67 | 4,3 | yellow | ||
| 22 | 7,3 | 5,03 | brown | ||
| 24 | 8,0 | 5,6 | blue |
Recovery after the procedure
The examination, which was carried out according to all the rules by a qualified gastroenterologist, does not require any recovery after its implementation.
After removing the probe, the patient is observed by the doctor for another hour. This is necessary in order to quickly and effectively eliminate possible negative consequences: injury to the esophagus or stomach.
Perforation of the stomach or injury to the mucous membrane can occur if the procedure is performed incorrectly. In this case, gastric bleeding often occurs. In this case, it is necessary to urgently take a number of actions:
- intramuscular injection of dicinone;
- intravenous injection of calcium chloride;
- blood transfusion (in case of large blood loss);
- applying ice to the stomach area.
Best materials of the month
- Coronaviruses: SARS-CoV-2 (COVID-19)
- Antibiotics for the prevention and treatment of COVID-19: how effective are they?
- The most common "office" diseases
- Does vodka kill coronavirus?
- How to stay alive on our roads?
In case of gastric perforation, urgent surgical intervention is necessary. However, such complications are extremely rare. This procedure almost always goes smoothly and painlessly.
Determination of early cancer of the esophagus and stomach
When treating early cancer of the stomach and esophagus using endoscopic methods, it is very important to understand what is hidden under the word “early”. The TNM staging system currently used in the United States for esophageal and gastric cancer focuses on the depth of tumor invasion (T), lymph node involvement (N), and the presence of metastases (M). Five-year survival rates vary depending on TNM stage. Cancer limited to the mucosa most often does not metastasize to the lymph nodes, but cancer involving the submucosal layer gives such metastases in 30% of cases [1]. Therefore, tumors limited to the mucosa can be removed endoscopically and serve as an alternative to surgical resection.
Possible complications after installation
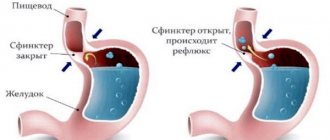
Any medical procedure is associated with risks. And even with full compliance with the technique of placing a nasogastric tube, complications cannot be ruled out. Most often, bleeding occurs due to damage to the mucous membranes during the passage of the tube through the passages or as a result of nasal bedsores. Non-serious complications also include throat diseases (pharyngitis, tracheitis), because the patient is forced to breathe through his mouth. Reflux esophagitis also often develops - the entry of gastric contents into the esophagus.
A more serious complication of probe installation is perforation (damage to the walls) of the esophagus, pneumothorax and infectious diseases in the form of abscesses of the larynx or retropharyngeal area. Such consequences require long-term treatment, up to the need for surgery.
The professionalism of the medical staff and full compliance with all the rules of the procedure will help to minimize the possibility of complications and increase the patient’s comfort during the installation of the probe. The patient himself can also contribute to all this by unquestioningly following medical recommendations.
In what cases is a gastric tube installed?
You don’t need to be a doctor to know approximately what a nasogastric tube is used for. Because its purpose is clear from the name itself. Translated from Latin nasus
- this is the nose, and
gastritis
from Greek - stomach. Those. The tube is passed through the nasal passages into the stomach so that food and medicine can be given through it in the future.
The main indication for the use of a tube is the inability to feed independently. And this can happen in different cases.
- Acute pancreatitis.
- Fistulas in the esophagus.
- The esophagus is narrowed enough to allow a thin tube to be inserted.
- Injuries to the abdomen, throat or tongue.
- The patient is in a coma.
- Refusal of food and vital medications due to mental disorders.
- Impaired swallowing function due to damage to nerve endings (this happens, for example, after a stroke).
- Postoperative period after surgical interventions on the stomach, intestines, pancreas.
By the way! Bringing food and medications into the stomach is not the only function of a nasogastric tube. It can also work in the opposite direction. And sometimes it is installed to drain the stomach cavity, i.e. to remove foreign fluids from it, for example, during or after abdominal operations on the gastrointestinal tract.
Feeding through a nasogastric tube.
The probe is lowered to the level of the stomach. Air should not be allowed to enter there. To do this, the funnel is tilted and filled with food. The food should be warm, its temperature should be 38-40 degrees. Once the funnel is filled with food, it is gradually raised up until the food remains only in the neck of the funnel. Next, the funnel descends again down to the level of the stomach. It is then filled with food and the process is repeated in a similar manner. After all the food has been introduced, boiled water or tea is poured into the tube.
After the introduction of food is completed and the probe is washed, a clamp must be installed on its end. Next, remove the funnel. Afterwards, wrap the end of the probe in a sterile napkin or place it in a tray, or you can fix it on the patient’s neck. Leave in this state until your next meal.