Removal of the stomach or gastrectomy is a traumatic procedure that is difficult for the patient and leaves lifelong complications, but stomach cancer has no chance of cure if surgery is not performed.
- Indications for gastric removal surgery for cancer
- How is the stomach removed for cancer?
- What is the best operational access when deleting?
- Stages of stomach removal
- Recovery after surgery
- Complications after cancer surgery
- Rehabilitation after stomach removal for cancer
- Prognosis after gastric removal
Before surgery, a cancer patient rarely thinks about how to live after removal of the stomach; it is important for him to quickly get rid of the tumor in order to survive. After surgical treatment, the understanding comes that the missing organ cannot be replaced with an artificial one, and health problems can no longer be avoided.
Indications for gastric removal surgery for cancer
Modern oncology strives to minimize the volume of tissue removed in order to minimize complications after surgery and subsequent suffering of the patient, however, complete removal of the stomach is one of the most common operations for cancer.
Gastrectomy is performed for tumors of both stages 1 and 3; an absolute contraindication for surgical intervention is the presence of distant cancer metastases.
Gastrectomy is performed when a smaller operation is not feasible or does not guarantee the absence of relapse. Gastrectomy is the last option for salvation; carcinoma cannot be cured in any other way.
Only in one case, with stage 4 gastric carcinoma, there is a relative contraindication to surgery - metastasis to the ovary. Relative because, if it is possible to remove the primary tumor and the ovary affected by metastases, two operations are performed simultaneously: gastrectomy and oophorectomy, sometimes together with the uterus. But if something cannot be removed, the surgical stage of treatment is replaced with chemotherapy.
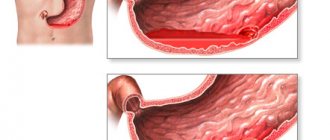
Gastric bypass according to Roux
Gastric bypass according to Roux
(OAZhR; English
Roux-en-Y gastric bypass
) is a surgical operation that reduces the volume of the stomach and divides the small intestine into two parallel sections. As a result of the operation, the volume of the stomach and the volume of absorbed nutrients are significantly reduced, which leads to a decrease in the patient’s weight. It is one of the main operations of bariatric surgery. In the first stage of the operation, a small pouch is created in the stomach using staples. The rest, the larger part of the stomach, is then separated from the small stomach, but not removed. At the second stage of the operation, the small intestine, where its first section, the duodenum, is adjacent to the second section of the small intestine, the jejunum, is divided into two parts. The jejunum rises and joins the newly created small stomach. The duodenum then joins the new intestinal branch, giving the intestine a Y shape. By bypassing the duodenum, the amount of nutrient absorption is significantly reduced, which leads to a significant reduction in the patient's weight. Roux-en-Y gastric bypass surgery results in a loss of 56.7–66.5% of excess weight in the first 24 months after surgery (K. Novak).
Complications after Roux-en-Y bypass surgery
The surgery may cause complications such as nausea, vomiting, and abdominal pain.
Gastrointestinal bleeding develops more often after Roux-en-Y bypass anastomosis. According to American data, gastrointestinal bleeding develops in 1.9% of cases. It can occur in a variety of locations, including the small stomach, anastomoses, non-operated portion of the small intestine, main stomach, or small intestinal bypass. About 20% of patients who have Roux-en-Y bypass surgery develop ulcers at the gastrojejunal anastomosis—most commonly in the first 3 months after surgery, but possibly at any other time. Postoperative anastomotic ulcers are treated with proton pump inhibitors. Bile reflux is treated with lipid-lowering drugs (cholestyramine and others). Patients should stop taking non-steroidal anti-inflammatory drugs, if possible, or combine them with taking proton pump inhibitors. One of the most serious complications after surgery is weight gain. About 20% of patients do not lose 50% of their excess weight within a year after surgery. In addition, 30% of patients regain weight within 2 years after surgery, and 63.6% within 4 years.
Publications for healthcare professionals addressing the issue of Roux-en-Y anastomoses
- Zherlov G.K., Kucherova T.Ya., Nustafaev R.S. Prevention and treatment of complications of gastric resection with Roux-en-Y anastomosis. Surgery. - No. 10. - 2004.
- Global practical recommendations of the World Gastroenterological Organization "Obesity". WGO, 2009..
On the website GastroScan.ru in the “Literature” section there is a subsection “Surgery of the stomach and small intestine”, containing articles for healthcare professionals.
The source of the “complications” section and figure is a publication by Kristine Novak. What are the Complications of Weight Loss Surgery? (https://agajournals.wordpress.com/2013/04/08/what-are-the-complications-of-weight-loss-surgery).
Back to section
How is the stomach removed for cancer?
The approach to the stomach through the abdominal wall - surgical access - depends on the patient’s condition and the extent of the tumor process in the esophagus. During the operation, the esophagus is crossed 5–7 centimeters above the tumor, the stomach and omental bursae with lymph nodes are completely removed. There should not be a single tumor focus left in the abdominal cavity.
Typical incisions of the skin and soft tissues of the abdomen:
- The classic incision is along the midline of the abdomen - this is a midline laparotomy.
- In some cases, they resort to extending the incision from the abdomen to the chest wall - this is a thoracolaporotomy.
- If it is necessary to remove a significant portion of the affected esophagus, in addition to the median laparotomy, an incision is made between the ribs.
- The esophagus affected by cancer can also be approached from the inside - through the diaphragm, which is also possible with classical access.
What is the best operational access when deleting?
There are no standards defining where and how much to cut the abdominal wall and how far to advance in the chest cavity; everything is based on the individual characteristics of the particular patient and the tumor lesion.
The oncologist surgeon independently chooses a surgical approach that, with maximum visibility of the field of activity, allows minimal damage to healthy tissue and the optimal surgical technique, which reduces the possibility of complications after removal of the stomach.
Today, in case of early cancer, open operations are successfully replaced by endoscopic technologies; laparoscopic gastrectomy is undoubtedly technically more difficult, but it is more beneficial for the patient, since it does not increase complications after the operation, and the patient’s recovery is faster.
The method of access to the diseased organ and the surgical technique are determined by the oncologist surgeon; his choice reflects practical surgical experience and personal skills; rest assured, the professional qualifications of our clinic’s specialists are always at the “top class” level.
Stages of stomach removal
The course of the operation to remove all or only part of an organ (resection) proceeds according to the same plan, but with a different volume of tissue removed.
- First, mobilization is carried out - cutting off the organ from the internal ligaments that fix it, ligating the supplying arteries and veins. At the same time, a thorough examination of the abdominal organs is carried out and, based on what is seen, adjustments are made to the operation plan.
- The second stage is the actual removal, with cutting off the stomach from the esophagus and duodenum. When nearby organs of the abdominal cavity are involved in the tumor conglomerate, including the diaphragm or liver, pancreas or large intestine, if technically possible, complex and extensive combined operations are performed, that is, gastrectomy and, for example, resection of the pancreas or liver.
- The third stage is the restoration of the digestive tract, that is, the connection of the esophagus with the intestines, which will ensure the further movement of food.
What is gastrectomy?
Resection (removal) of the stomach (code according to the international classification of diseases K91.1) is necessary when conservative treatment methods become powerless. It is prescribed to patients diagnosed with cancer, peptic ulcers, polyps and other diseases of the gastrointestinal tract. Gastric surgery is performed in several ways:
- Partial resection of the lower part of the stomach, when the preserved part is connected to the duodenum.
- Partial resection of the upper part of the stomach, when the upper area, which is involved in the pathological process, is excised, and then a subsequent connection of the esophagus is made to the lower part of the organ.
- Sleeve (longitudinal) gastroplasty. This type of operation is used in the treatment of obesity, when most of the stomach is removed while preserving the natural connections of the duodenum and esophagus.
- Complete gastrectomy, when the entire organ is removed and then a connection is made between the duodenum and the final part of the esophagus.
Recovery after surgery
Stomach cancer leads to serious intracellular changes; all biochemical processes are disrupted, since the body does not receive the substances it needs due to impaired absorption in the gastrointestinal tract. A few decades ago, every fourth patient died after gastrectomy; today complications and mortality are reduced to minimal levels.
Postoperative recovery is very individual; it is affected by the age and gender of the patient, his existing chronic diseases and the degree of impairment caused by carcinoma, the involvement of other abdominal organs and the “live” weight of the patient. Even the time of year affects the duration of recovery; summer is not the most favorable time for surgical procedures.
The main thing for the patient is not to rush to leave the clinic after removal of the stomach, since incomplete treatment measures will subsequently result in health problems that can completely ruin life.
Indications for surgery
Absolute indicators for resection are malignant tumors of the stomach, when surgery gives the patient a chance to prolong life. Doctors prescribe surgical intervention when ulcers do not heal for a long time, the acidity of gastric juice is reduced, or severe scar changes occur that give a pronounced clinical picture.
Stomach cancer
All organs of the human body are made up of cells that grow and divide when new cells are needed. But sometimes this process is disrupted and begins to proceed differently: cells begin to divide when the body does not need it, and old cells do not die. Additional cells accumulate, forming tissue that doctors call a tumor or neoplasm. They can be benign or malignant (cancerous).
Stomach cancer begins in the inner cells, but over time invades the deeper layers. In this case, the tumor can grow into neighboring organs: the esophagus, intestines, pancreas, liver. The causes of malignant neoplasms of the stomach are divided into several types:
- poor nutrition, especially associated with the abuse of fried, canned, fatty and spicy foods;
- smoking and alcohol;
- chronic diseases of the gastrointestinal tract: ulcers, gastritis;
- hereditary predisposition;
- hormonal activity.
Severe stomach ulcer
An ulcer is a defect in the gastric mucosa. Peptic ulcer disease is characterized by periodic exacerbations, especially in the spring and autumn. The main reason for the development of the disease is frequent stress, which strains the nervous system, which causes muscle spasms in the gastrointestinal tract. As a result of this process, a malfunction in the nutrition of the stomach occurs, and gastric juice has a detrimental effect on the mucous membrane. Other factors leading to the development of peptic ulcers:
- disrupted diet;
- chronic gastritis;
- genetic predisposition;
- long-term medication use.
With a chronic gastric ulcer, the formation of ulcerative defects occurs on the mucous membrane of the organ. Resection of these pathologies is performed when complications of the disease develop, when there is no effect from conservative therapy, bleeding occurs, and stenosis develops. This is the most traumatic type of surgery for stomach ulcers, but also the most effective.
- 3 common myths about gasoline for cars
- Benefits for medicines for pensioners - list of free and discounted ones, compensation for refusal
- Alimony for parents of pre-retirement age
Laparoscopic resection for obesity
Laparoscopic surgery is an endoscopic method of gastric surgery, which is performed through punctures in the abdominal cavity with a special instrument without a wide incision. This resection is carried out with the least trauma for the patient, and the cosmetic postoperative result is much better. The indication for laparoscopic gastrectomy is the extreme stage of obesity, when neither medication nor a strict diet helps the patient.
With obesity, a metabolic disorder occurs, and when the process of losing weight can no longer be controlled, doctors have to remove part of the stomach, after which the patient gets rid of the problem, loses weight and gradually returns to everyday life. But the biggest advantage of laparoscopy is the restoration of normal metabolism, reducing the risk of atherosclerosis and coronary heart disease. Watch the video to see how laparoscopic gastrectomy is performed:
Complications after cancer surgery
Early complications are few, but if not detected in time, they can be fatal for the patient.
The failure of the sutures at the junction of the esophagus with the intestine - at the anastomosis - does not arise because the surgeon “did something wrong”, but is due to the insufficiency of the body’s internal reserves, homeostasis disorders, weakness of the immune defense and inadequate nutrition - nutritional status before treatment. The incidence of this complication ranges from 2% to 10%.
Impaired outflow of pancreatic secretions due to swelling of the pancreas can lead to the development of acute pancreatitis. The incidence of pancreatitis is affected by surgical technique, but the determining role is played by the volume of tissue removed and the initial condition of the gastrointestinal tract. The main thing is to diagnose the complication in time and carry out adequate drug prevention.
Failure of sutures and pancreatitis can initiate inflammatory processes inside the abdominal cavity, in particular, an abscess or peritonitis, intestinal obstruction or local accumulation of fluid.
The percentage of the listed pathological postoperative conditions is small, and in our clinic it is significantly lower than the average statistical values, because the result reflects the talent and experience of the oncologist surgeon in combination with excellent diagnostic capabilities.
Basic methods of performing the operation
There are many different options for gastric resection and reconstruction. Theodor Billroth first performed such an operation back in 1881, and in 1885 he also proposed another way to restore the functioning of the gastrointestinal tract. These gastric surgeries are still used today, but today they have been modernized and simplified, so they are available to a wide range of practicing surgeons. The doctor selects the type of operation individually in each case, but more often they use:
- Subtotal distal resection, when the lesion is located in the pyloroantral part of the lower third of the stomach (the entire lesser curvature).
- Subtotal proximal resection, performed for stage 1 and 2 gastric cancer, when the lesser omentum, lymph nodes, lesser curvature and a section of the greater omentum are removed.
- Gastrectomy, which is performed in the presence of a primary multiple tumor or infiltrative cancer located in the middle part of the stomach. The entire organ is removed, and an anastomosis is performed between the esophagus and the small intestine.
By Billroth 1
Gastric resection according to Billroth 1 is the excision of 2/3 of the organ, when the physiological path of food movement with the participation of pancreatic excretion and bile is preserved. During surgery, the anastomosis of the duodenum and stomach is connected end to end. This method is used for polyps, malignant ulcers, and small cancerous tumors of the gastric antrum.
- Salad with sprats - how to prepare according to simple and tasty step-by-step recipes with photos
- Stretching and flexibility exercises
- Meatballs in a slow cooker
By Billroth 2
During Billroth 2 resection, a large part of the blind stump of the duodenum and stomach, anterior and posterior anastomosis (connection of two organs) are removed. After this operation, the physiological path of food movement is disrupted - it enters directly into the jejunum, and bile reflux is possible and the anastomosis is disrupted. Resection according to Billroth 2 has more indications, since it is performed on gastric ulcers of any location and for cancer, since it gives the doctor the opportunity to perform extensive removal of the organ up to 70%.
According to Hoffmeister-Finsterer
The Hofmeister-Finsterer technique is a modified version of Billroth 2, which provides for resection of at least 2/3 of the organ for peptic ulcer disease. During the operation, the entire secretory zone is removed, after which the motor function of the stomach undergoes significant changes: peristalsis weakens, the function of the pylorus, which ensures the gradual evacuation of food, disappears altogether.
By Ru
The Roux method is the removal of part of an organ with a Y-shaped gastroenteroanastomosis. In this case, the jejunum is divided, and its distal end is sutured and connected to the lower third of the gastric stump. This is also a modification of Billroth 2, which is indicated for duodenogastric reflux esophagitis, which is characterized by the reflux of the contents of the duodenum into the stomach.
According to Balfour
The Balfour method involves placing a gastrointestinal connection on a long loop of jejunum. This method prevents pathological changes in the organs of the gastrointestinal tract, and is also used for very high resection due to peptic ulcer or the impossibility of suturing in another way due to the anatomical features of the gastric stump. Balfour resection eliminates the gap between the knees of the jejunum, which eliminates the future occurrence of intestinal obstruction.
Rehabilitation after stomach removal for cancer
It is impossible to overestimate the importance of restorative measures after gastrectomy; by and large, good health “comes” to the patient a month after discharge from the hospital. If we try to briefly answer the question “how do they live after removal of the stomach,” then it definitely doesn’t matter when they live without the help of specialists.
The wound will heal, but restoration of normal nutritional status in the altered digestive tract is difficult - simply pureed and steamed food does not solve the problem. And the problem is associated with a lack of immunity and the lack of complete absorption of nutrients necessary for the body.
For a speedy recovery and continuation of antitumor treatment, an individual rehabilitation program is required.
Prognosis after gastric removal
Oncological statistics know how long patients with gastric carcinoma live, depending on the stage. There is no literature data on whether removal of the most important part of the digestive tract shortens life, but it is known for sure that the patient’s life expectancy depends on the prevalence of primary carcinoma and the biological characteristics of cancer cells - differentiation, their sensitivity to chemotherapy and concomitant diseases.
Oncological science is very precise, it knows what diagnostic algorithm is needed for the disease, what percentage of patients at different stages and how many years they live on average, and can offer a whole range of therapeutic measures for certain morphological characteristics of carcinoma.
There is one thing that oncology cannot do - give a specific patient a prescription for optimal treatment with an exact schedule of the manipulations and procedures he needs. But experienced oncologists at the European Clinic can and do do this.
| More information about the treatment of stomach cancer at the European Clinic: | |
| Treatment of stomach cancer | |
| Oncologist-gastroenterologist | 5100 rub. |
| Chemotherapy appointment | 6900 rub. |
| Emergency oncology care | from 11000 rub. |
Book a consultation 24 hours a day
+7+7+78
Bibliography
- Davydov M.I., Turkin I.N., Polotsky B.E./Modern surgery of gastric cancer: from D2 to D3//Proceedings of the IX Russian Oncological Congress; Moscow 2005.
- Stilidi I.S., Nered S.N./Modern ideas about the basic principles of surgical treatment of locally advanced gastric cancer // Practical Oncology; 2009; T.10, No. 1.
- Yankin AB/Modern surgery of gastric cancer //Practical Oncology; 2009; T. 10, No. 1.
- Curcio G., Mocciaro F., Tarantino I. et al./Self-Expandable Metal Stent for Closure of a Large Leak after Total Gastrectomy //Case Rep. Gastroenterol.;2010; No. 4.
- Etoh T., Inomata M., Shiraishi N., Kitano S./Revisional Surgery After Gastrectomy for Gastric Cancer //Surg. Laparosc. Endose. Percutan. Tech.;2010.;v. 20, no. 5.
- Isgiider AS, Nazli O., Tansug T., et al/ Total gastrectomy for gastric carcinoma// Hepatogastroenter.; 2005; v. 52.
- Zhang CH, Zhan WH, He YL et al. /Spleen preservation in radical surgery for gastric cardia cancer //Ann. Surg. Oncol.; 2007; v. 14.