In what cases is a gastrostomy tube placed?
Gastrostomy placement is indicated for the following conditions:
Permanent gastrostomy:
- Inoperable tumor of the pharynx or esophagus.
- Tumor of the mediastinum compressing the esophagus.
- Tumor of the inlet of the stomach.
- Cicatricial narrowings of the esophagus that cannot be bougienaged.
- Patients with damage to the nervous system whose swallowing reflex is impaired (patients with stroke, myasthenia gravis, amyotrophic lateral sclerosis, brain tumors).
A permanent gastrostomy can provide the patient with almost complete enteral nutrition, and for a long time. It can be classified as palliative surgery - it prolongs a person’s life without eliminating the underlying problem. The quality of life, of course, deteriorates, but mainly not because of the presence of gastrostomy, but because of the underlying disease.
Temporary gastrostomy:
- Chest wounds with damage to the esophagus.
- Severe maxillofacial injuries.
- Esophageal-tracheal or esophageal-bronchial fistula.
- Burns of the esophagus during healing and restoration of patency.
- In some cases, after extensive abdominal surgery (gastric resection, elimination of acute intestinal obstruction) for decompression and aspiration of gastric contents.
- For the period of preparation for operations on the esophagus or stomach in severely malnourished patients, if it is obvious that this period will be long enough.
Temporary gastrostomy allows you to provide adequate nutrition for a period of temporary inability to eat naturally. A temporary gastrostomy is formed in such a way that it can be removed in the future without repeated extensive surgery.
Diseases leading to surgery
Surgical intervention to place a gastrostomy is often used in oncology for inoperable tumors. Neurological patients may need it to ensure the supply of nutrients. Diseases that lead to the need to insert a gastrostomy tube are as follows:
- inoperable tumors with metastases in the esophagus, mediastinum, lungs, larynx, oral cavity;
- trauma, injury to the esophagus, face, jaws, as well as brain tissue, centers that regulate the swallowing process;
- developmental pathologies;
- formation of tracheoesophageal fistula;
- stroke complicated by dysphagia;
- amyotrophic lateral sclerosis, according to ICD code G 12.2, etc.
For some diseases of the central nervous system, senile diseases, as well as for severe, bedridden patients, an ostomy may also be indicated.
Types of gastrostomy
Today, there are about 100 different methods of applying gastrostomy. The main essence of the operation is the formation of a fistula connecting the stomach cavity with the environment.
Operations where the hole in the stomach was simply sutured to the skin, as with a colostomy, are a thing of the past. Their main drawback: the contents of the stomach constantly poured out.
It is necessary to form a tunnel, which will serve as a fistula. It is also advisable to create some semblance of valves along the fistula. A tube with a diameter of about 8 mm made of PVC or rubber is inserted into this tunnel. The tube is inserted into the opening of the fistula for each feeding, or it is placed immediately during the formation of the gastrostomy and remains there permanently.
In various techniques, a gastrostomy fistula can be formed from the walls of the stomach, cut from flaps of the stomach wall, from a skin flap, or a section of the small intestine can be used for these purposes.
The most common types of gastrostomy at present are gastrostomy according to Witzel, according to Stamm-Kader, and also according to Topver.
Possible complications
For 24 hours after surgery, the gastrostomy opening is kept open to monitor the functionality of the stomach. In the next 10 days, it is possible that a number of different complications will develop, the relief of which may require emergency medical care:
- Acute pain after the effect of anesthesia wears off.
- Development of peritonitis.
- Bleeding, which can also affect the stomach cavity.
- Multiple purulent formations in meristematic tissues.
- Deformation of the walls of the stomach, which may require repeated surgery.
- Hernia of the anterior abdominal wall.
- Maceration of the skin and dermatitis along the entire perimeter of the gastrostomy.
- Probe falls out.
Today, gastrostomy surgery is considered one of the easiest. But medical statistics show that in 3% of cases patients die.
In more than 92% of all situations, complications in the postoperative period occur due to poor gastrostomy tightness. In this case, the injected nutritional mixtures and gastric juice leak into the sutured wound, causing suppuration to form and an inflammatory process to develop.
Gastrostomy can be performed urgently for those patients who are severely weakened and dehydrated. If the patient is exhausted, then the nutritional mixture is administered through a tube immediately after surgery, but only dropwise (maximum 100 drops per minute). Doctors must monitor the process of gastric emptying, which is why the tube must be open.
Fractional meals for malnourished patients are available only from the second day after gastrostomy. To reduce the likelihood of wound infection and the development of various complications, doctors follow a clear algorithm for patient care. If all the rules are followed, the postoperative wound heals, and the patient quickly recovers.
Preparation for gastrostomy surgery
Gastrostomy is a palliative operation performed for life-saving reasons. The main contingent of patients are weakened, exhausted cancer patients. We can say that the only contraindication for it is the agonal state.
In other cases, with an insufficiently compensated condition, preoperative preparation is carried out:
- Fluid losses during hypovolemia are replenished. To do this, saline solution and 5% glucose solution are infused intravenously. Monitoring is carried out based on the level of central venous pressure, diuresis, and hematocrit level.
- Correction of electrolyte disturbances under the control of analysis of basic plasma electrolytes.
- Replenishment of protein deficiency by parenteral nutrition (transfusion of protein hydrolysates, amino acid solutions, plasma) or enteral nutrition through a nasogastric tube.
- For anemia, blood or red blood cell transfusions are possible.
- The maximum possible compensation of cardiac and respiratory function.
- Laparocentesis for ascites.
- Psychological preparation of the patient: he must clearly imagine his future life with a gastrostomy and not be afraid of it. In some cases, patients refuse such surgery due to insufficient information about it.
- If the esophagus is passable for a nasogastric tube, aspiration of gastric contents and gastric lavage are performed immediately before surgery.
Gastrostomy can be a separate operation or part of another extensive operation.
Gastrostomy according to Witzel
Today, the most commonly used is gastrostomy according to Witzel:
- Usually performed under general anesthesia. In very weakened patients, it can be performed under local infiltration anesthesia.
- Position – on the back, with the leg end slightly lowered. This is necessary so that the stomach, which is usually tucked up in such patients, drops below the costal arch.
gastrostomy according to Witzel
Incision - on the left in the middle of the rectus abdominis muscle downwards, 4-5 cm long.- The skin, muscle, aponeurosis, and peritoneum are dissected layer by layer.
- The stomach wall is removed into the wound.
- A tube is laid along its central axis in an obliquely ascending direction. The end of the tube should be projected onto the air bubble in the cardiac region.
- The tube is sutured on top with serous-muscular sutures to a length of 5-7 cm. A stapler can also be used for these purposes. The folds of the serous membrane over the tube should be closed until the edges completely touch. Thus, a tunnel is formed.
- A purse-string suture (circular) is placed around the end of the tube. A puncture is made inside the stomach wall, and the tube is inserted inside through this puncture. The purse string suture is tightened. Several more stitches are placed on top of it to secure it.
- The parietal peritoneum in the area of the immersed tube is sutured in a circle to the stomach. The rest is sewn together with a continuous seam. A tightness of the abdominal cavity is created.
- Gastropexy - the stomach is sutured to the abdominal wall with several sutures without any tension.
- The outer end of the tube is brought out either through the main incision or (more often) slightly to the side of it, for this a separate puncture is made.
- The wound is sutured layer by layer.
- The tube brought out is clamped with a clamp or closed with a special plug.
Video: example of gastrostomy according to Witzel (on a rabbit)
Gastrostomy according to Stamm-Kader
The principle of the operation is also to create a tunnel for the tube from the walls of the stomach, but in this case it is not obliquely ascending, but perpendicular to the wall of the stomach.
- The cut is similar to the first method.
- The anterior wall of the stomach is stretched with holders like a cone. Three purse string sutures are placed on the elongated part, at a distance of 2 cm from each other, without tightening the threads.
- A small incision is made at the top of the cone and a tube is inserted. The first suture is tightened first, the tube is invaginated inward, then the second and third sutures are tightened alternately. It turns out a straight channel formed inside by the serous membrane of the stomach with a rubber tube located in it.
- The stomach is sutured to the abdominal wall.
- The wound is sutured layer by layer, leaving the end of the tube outside.
Both of these methods are more suitable for placing a temporary gastrostomy. The gastrostomy channel is lined from the inside with a serous membrane, which can be soldered if the tube is removed.
If there is no longer a need for a gastrostomy tube, the tube is removed without repeated surgery, and the fistula gradually heals on its own. However, this advantage becomes a disadvantage in another situation: if the tube accidentally falls out of the channel, it will be difficult to reinsert it into place.
Gastrostomy according to Topver
This is already a method of applying a permanent gastrostomy:
- Left-sided transrectal access.
- A cone is pulled from the anterior wall of the stomach into the surgical wound.
- Just as with the Kader technique, three layers of purse-string sutures are applied to it.
- A hole is made at the top of the cone and a rubber tube is inserted inside. Purse string sutures are tightened. After layer-by-layer suturing of the wound, the tube is removed, and the edges of the gastric opening are sutured to the skin.
- As a result of this operation, a labiform fistula is obtained with corrugated walls formed not from the serous, but from the gastric mucosa. These folds prevent the contents of the stomach from leaking out. A tube is inserted into the resulting hole at each feeding, and after feeding it is removed.
gastrostomy according to Topver
This gastrostomy will not heal on its own. If there is a need to eliminate it, you will have to do a second operation.
Video: example of installing a permanent gastrostomy tube
Checking the probe's serviceability
Caring for a gastrostomy tube (the algorithm of actions must be clarified with the attending physician, since if the dressings are changed incorrectly, there is a possibility of infection of the wound and stomach tissues) involves daily checking the serviceability of the tube.
Otherwise, it will be difficult to ensure smooth passage of food into the stomach. Incorrect position of the gastrostomy tube can cause acute pain.
There are two ways to verify that the probe is working:
- It is necessary to check the correct positioning of the disc for external fixation.
- Measure the acidity of the stomach contents.
Experts prefer to use the second option, as it makes sure that the gastrostomy is applied correctly and will not cause pain to the patient.
Acidity test
To check acidity, you need to prepare a syringe, warm water and indicator paper.
The procedure is carried out in stages:
- You need to wash your hands and treat them with an antiseptic. It is necessary to remove the tip from the probe and install a syringe in its place.
- You need to pull the syringe plunger as smoothly as possible to draw a little liquid. It is forbidden to make sudden movements that can injure the stoma and the gastric mucosa.
- After disconnecting the syringe from the probe, close the tip.
- Apply a drop of liquid from a syringe to the prepared indicator paper.
If the acidity level of the stomach contents is within the 5.5 mark, then the probe is installed correctly, so it can be rinsed with a small amount of warm water and begin feeding food or medications.
If the indicator is too high, then you need to wait at least 30-70 minutes. If even after this time the acidity level has not decreased, then using the probe is prohibited, since only a qualified doctor can correct the situation.
When to ask for help
A patient with a gastrostomy should urgently seek medical help in the following cases:
- The probe sank too deeply into the stomach.
- Rashes and purulent discharge appeared on the skin around the gastrostomy tube.
- The tube fell out. If the patient does not immediately contact the attending physician, then after 4-6 hours the stoma opening will close.
- Painful sensations appeared in the gastrostomy area.
It is best to buy a spare tube in advance for timely administration of food and medications, so that, if necessary, you can quickly replace a failed product.
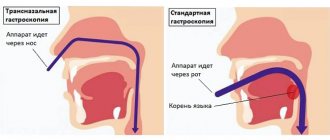
Endoscopic gastrostomy
There is a technique for percutaneous endoscopic gastrostomy. The main condition for this is the patency of the esophagus so that an endoscopic tube can be inserted. This intervention does not require general anesthesia and is quite simple at first glance: a gastrostomy tube is inserted through a small puncture of the abdominal wall.
However, this operation is quite difficult for surgeons and requires honed skills. Performed by two surgeons.
An endoscope is inserted through the esophagus into the stomach. Under visual control, the doctor selects an area on the anterior wall of the stomach that is most suitable for a puncture and presses the end of the endoscope into it.- Another surgeon finds this place from the outside, palpating the abdominal wall. For better visualization, the lights in the operating room are turned off so that the illuminated end of the endoscope is visible.
- Local anesthesia is performed with a solution of novocaine or lidocaine.
- From the outside, the abdominal wall and the wall of the stomach are pierced with a trocar, and a conductor (thread) is inserted into its lumen. Using an endoscope, the thread is captured and removed through the mouth.
- A gastrostomy tube is attached to the end of the thread.
- Along the guidewire, the tube is inserted into the stomach.
- Using an endoscope, the correct installation is checked.
- The tube is fixed.
Video: description of gastrostomy installation under endoscopic control
What is a gastrostomy
Gastrostomy (GS) is a surgical opening in the wall of the stomach, connecting its cavity with the external environment through the anterior abdominal wall. GS makes it possible to introduce food into the gastrointestinal tract directly through it, bypassing the oral cavity and esophagus.
A gastrostomy tube is installed during a special operation (gastrostomy), performed under short-term general anesthesia or local anesthesia. A plastic (silicone) tube is inserted into the hole in the front wall of the stomach and extends outward. It serves as a channel through which food is introduced. Using locking discs, the probe is secured in a certain position relative to the abdominal wall.
The presence of valves prevents the uncontrolled flow of contents from the stomach to the outside. The outer end of the HS, closed with a special valve, is fixed to the skin of the abdomen. The operation time is no more than 20 minutes.
More than 100 methods of installing a gastrostomy tube have been developed, but two are most widespread:
- X-ray controlled gastrostomy (X-ray controlled gastrostomy). Performed in patients with respiratory failure, especially severe in the supine position. The operation is performed with the patient in a sitting position. The disadvantage of the method is weak fixation of the stomach, which can lead to the penetration of digestive juices into the subcutaneous tissue and abdominal cavity. GSR has been used quite rarely in recent years.
- Percutaneous endoscopic gastrostomy (PEG). In this case, a hole in the anterior abdominal wall and stomach is made percutaneously. The formation of a gastrostomy occurs under the control of an endoscope inserted into the stomach through the esophagus. This is the most commonly used and low-traumatic method, but its use is impossible in case of esophageal obstruction.
Indications and contraindications for gastrostomy
A gastrostomy can be installed for both temporary and permanent use. This operation does not affect the underlying disease, but provides adequate nutrition to the patient, improving the quality of life. Such treatment methods are called palliative.
Main indications for installing a permanent HS:
- narrowing of the esophagus that cannot be corrected;
- inoperable cancer of the pharynx and esophagus;
- external compression of the esophagus (for example, with tumors of the mediastinum);
- impaired swallowing reflex in neurological diseases (stroke, amyotrophy, severe forms of cerebral palsy, brain tumors).
The need to form a temporary GS arises in the following cases:
- injuries to the esophagus (burns, wounds) for the time necessary for full recovery;
- severe damage to the face and jaw apparatus;
- esophageal fistula;
- extensive abdominal surgery to decompress the stomach and pump out its contents;
- in the preoperative period before interventions on the gastrointestinal tract for enhanced nutrition of patients with extremely low body weight.
Contraindications for surgical treatment:
- the patient is on peritoneal dialysis;
- the presence of fluid in the abdominal cavity (ascites);
- enlarged liver and spleen;
- high degree of obesity.
Immediately after surgery
Immediately after the gastrostomy tube is installed, parenteral nutrition continues for 24 hours. The next day, a small amount of saline is injected with a syringe to rinse and check the patency of the tube.
On the first or second day, the patient is given small portions (50-100 ml) of glucose solution, saline solution, and unsweetened decoctions of dried fruits. The volume of liquid should not exceed 1 liter per day.
If patency is normal and there is no regurgitation, on the third day you can introduce diluted meat broth (300 - 500 ml).
During the first week, it is advisable to introduce food using a syringe, very slowly.
If there are no complaints, you can add liquid pureed porridge with water to your diet. Administer the porridge in portions of no more than 70 ml at a time. The total volume per day is 400-500 ml. At the same time, the introduction of compote, light tea without sugar and broth continues.
Gradually, the volume of food is increased to 1500 ml by the end of the week, the amount of a single serving also gradually increases (up to 180 ml).
You do not need to shower or bathe for a week after your gastrostomy.
With a permanent gastrostomy tube, the gastrostomy tube is not removed until the wound has completely healed.
Solving possible problems with gastrostomy:
Gastrostomy blockage:
If power does not pass into the tube or is inserted with force, the tube is clogged. The blockage of the tube can be cleared with boiled water or pancreatin solution, injecting it for 1 hour. You can also use a soda (cola) solution. This solution is injected into the tube for 20 minutes.
Stoma leakage:
- This is normal if a gastrostomy tube has been installed recently. Within a month after installation, the gastrostomy tube may leak. It is necessary to change the feeding position and this problem may disappear.
- The external fastening of the tube or its integrity is damaged. In this case, it is necessary to replace the tube. Also, tubes are replaced in accordance with their service life. Percutaneous endoscopic tubes are replaced approximately every 1-2 years. Balloon gastrostomies are changed every 3-6 months. (Unless otherwise recommended by your doctor).
- Bloating, irregular bowel movements (less than once every 2-3 days). It is necessary to adjust the diet. Consult your doctor for additional recommendations.
Important! In other cases, you should consult a doctor, as leakage may be due to serious reasons: infection, decreased gastric motility, or increased secretion.
Changing the lock position:
If the clamp disk is too deep, loosen the clamp slightly by moving the disk towards you relative to the tube. The pressure of the fixative on the skin can lead to inflammation.
Nutrition through a gastrostomy tube
By the time of discharge (10-14 days after surgery), the volume of nutrition is increased to 2 liters per day, the number of feedings is reduced, food is administered using a funnel attached to the outer end of the tube. The patient learns to do this independently or with the help of relatives.
feeding through a gastrostomy tube
Products that can be introduced through a gastrostomy tube: pureed soups, porridges, meat and fish broths, milk, kefir, yogurt, fruit and vegetable purees, raw eggs, tea, compote, jelly.
Food should be warm, not hot or cold.
Special mixtures for enteral nutrition are also produced, balanced in the composition of nutrients and enriched with vitamins and microelements.
After adaptation, 5-6 feedings per day are usually required, the volume of one serving is 300 - 400 ml. This is the so-called bolus nutrition.
Sometimes bolus feeding is poorly tolerated, especially in severely bedridden patients. Then continuous nutrition is prescribed: the food mixture is introduced slowly continuously using a special dispenser or pump.
Before and after each feeding, the tube must be rinsed with saline or plain still water using a syringe.
If a permanent tube is installed, after feeding it is clamped or closed with a special stopper. The end of the tube is usually secured to the skin with an adhesive tape or another method of securing it (with a belt).
If the patient can chew, he can be given a small portion of food to chew to obtain a taste sensation and increase gastric secretions. After chewing, the food is spat out.
When maceration (wetting) of the skin around the fistula occurs, it is treated with antiseptics, zinc or other ointment is applied, and a sterile napkin is applied.
The structure of a modern gastrostomy tube
There are many types of gastrostomy tubes. The main components that a tube should consist of for ease of use:
- The tube itself.
- Internal fixation block (usually a small container filled with liquid through a separate portal at the outer end of the tube).
- External fixation device.
- Anti-reflux valve.
- Clamp.
- Cork.
There are types of gastrostomy for active patients - they are practically invisible on the body and do not limit normal physical activity in any way.
Gastrostomy tubes are quite expensive (the minimum price starts from 50 euros). Therefore, in the absence of a special device as a gastrostomy, it is possible to install a conventional Foley catheter, which is designed according to the same principle.
Pros and cons of installing a gastrostomy tube
Gastrostomy allows you to prolong the patient’s life. An alternative to gastrostomy tube feeding is nasogastric tube feeding. It can be installed in seriously ill patients for the same purpose - providing nutrition. However, this method has its drawbacks:
- It cannot be installed in case of complete obstruction of the esophagus.
- If the probe is in place for a long time, complications are possible: aspiration pneumonia, bedsores of the esophagus, infectious complications in the nasopharynx.
- Causes a lot more inconvenience.
Gastrostomy is also not without its disadvantages; if gastrostomy persists for a long time, complications are possible:
- Infection of the abdominal cavity.
- Infection of the skin around the stoma.
- Cutting purse string sutures.
- Bleeding.
However, with proper care, the functioning of a gastrostomy tube is still much more convenient than tube feeding.
Daily care algorithm
Gastrostomy tube care should be especially careful during the first two weeks after surgery. Experts recommend adhering to a clear algorithm of actions to prevent pathogens from entering the wound:
- The first step is to thoroughly wash your hands with soap, treat them with an antiseptic and put on sterile gloves.
- You should open the disk, which is responsible for fixing the gastrostomy, with smooth movements in order to loosen it a little. It is necessary to ensure that the safety element (clamp) does not change its position.
- Using boiled water, you need to clean the skin around the stoma and under it. This is recommended to be done in the morning and evening.
- The gastrostomy tube must be smoothly rotated 180 degrees. Thanks to this, the medical device can be avoided from sticking to tissues.
- After each administration of food and medications, the probe should be thoroughly washed using clean boiled water.
During the period of stoma care, it is recommended to avoid using gels and creams, as there is a high probability of damage to the gastrostomy. It is best to give preference to the antiseptic solution Polyhexanide.
Recommendations
For comprehensive gastrostomy care, the following recommendations should be taken into account:
- It is forbidden to treat the skin with a piece of gauze or bandage. These materials can leave small villi and fibers on the treated area, which can cause irritation of the epithelium.
- It is not recommended to apply hormonal cream or ointment to the skin around the stoma without your doctor's instructions.
- It is strictly forbidden to attach a bandage or adhesive tape over the gastrostomy tube. Otherwise, pathogenic microorganisms may penetrate into the wound, which will provoke tissue inflammation with the formation of exudate.
- Hydrogen peroxide and talc should not be used to treat the skin around the gastrostomy tube. These products can cause rashes on the skin.
Balloon types of gastrostomy should be changed every 5 months, and percutaneous types - once every 2 years.